You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Influence of Parental Separation and Its Health ImplicationsDocument60 pagesInfluence of Parental Separation and Its Health ImplicationsOmobomi SmartNo ratings yet
- (USCG Cert) 162.060.7.1 - Techcross - Aprill30 - 2019Document2 pages(USCG Cert) 162.060.7.1 - Techcross - Aprill30 - 2019peter1070811No ratings yet
- Onshore Knockout Drum GuidanceDocument2 pagesOnshore Knockout Drum Guidanceneil_nhNo ratings yet
- Vedic Mantras An Influential Factor For Spiritual HealthDocument7 pagesVedic Mantras An Influential Factor For Spiritual Healthbanny 123No ratings yet
- Psychiatry Research: SciencedirectDocument6 pagesPsychiatry Research: SciencedirectAmaury Enrique Frias DotelNo ratings yet
- A Single-Cell Atlas and Lineage Analysis of The AdultDocument17 pagesA Single-Cell Atlas and Lineage Analysis of The Adult奕蓁陳No ratings yet
- Sub Bituminous Coals An OverviewDocument91 pagesSub Bituminous Coals An OverviewBEN DUNCAN MALAGA ESPICHANNo ratings yet
- Instruction Det 5 - 3D PDFDocument59 pagesInstruction Det 5 - 3D PDFhafiziNo ratings yet
- Essential of PharmacoeconomicsDocument5 pagesEssential of PharmacoeconomicsNguyen Thi Thu Thuy25% (4)
- Gsef 2021 Research Plan Project Summary InstructionsDocument1 pageGsef 2021 Research Plan Project Summary Instructionsapi-550508557No ratings yet
- Symbol of Quality: Pioneers in Solderless Terminals, Crimping Tools & Cable GlandsDocument27 pagesSymbol of Quality: Pioneers in Solderless Terminals, Crimping Tools & Cable Glandsanbu selvanNo ratings yet
- Jihad-al-Nikah or Sex Jihad: 10 Interesting FactsDocument2 pagesJihad-al-Nikah or Sex Jihad: 10 Interesting FactsShyam Dass GuptaNo ratings yet
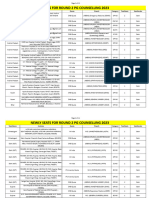
- Newly Seats For Round 2 PG Counselling 2023Document11 pagesNewly Seats For Round 2 PG Counselling 2023Manoj KumarNo ratings yet
- Contract Employment DetailsDocument2 pagesContract Employment DetailsLàtishà Puràñ67% (3)
- Smoke PointDocument16 pagesSmoke PointSuhaib IqbalNo ratings yet
- CE 132 - Geotechnical Engineering 2Document38 pagesCE 132 - Geotechnical Engineering 2hahaduNo ratings yet
- United States Bankruptcy Court District of Colorado Voluntary PetitionDocument64 pagesUnited States Bankruptcy Court District of Colorado Voluntary Petitionspacecat007No ratings yet
- FY2011 AnnualPlanDocument184 pagesFY2011 AnnualPlanCity Limits (New York)No ratings yet
- Servuction ModelDocument10 pagesServuction ModelMalik zainNo ratings yet
- Act 631 Finance Act 2003Document20 pagesAct 631 Finance Act 2003Adam Haida & CoNo ratings yet
- Module 1 - Lecture 2Document32 pagesModule 1 - Lecture 2Bruce bannerNo ratings yet
- 628c4fc51435e Chemical Engineering Pre Board Exam Day 2 Answer KeyDocument10 pages628c4fc51435e Chemical Engineering Pre Board Exam Day 2 Answer KeyKimNo ratings yet
- InfluenzaDocument106 pagesInfluenzaAmit Ramrattan100% (3)
- The Rights and PrivilegesDocument50 pagesThe Rights and PrivilegesM'dth Cal100% (2)
- Plant PartsDocument49 pagesPlant Partsshahzad18400% (1)
- 08.2279 USD2461b (1) Supor EKV BRODocument16 pages08.2279 USD2461b (1) Supor EKV BROMichał KoczorowskiNo ratings yet
- Al Ansari Profile OmanDocument24 pagesAl Ansari Profile OmanMohamed RusfanNo ratings yet
- BBB Vs AAA. GR 193225 February 9, 2015docxDocument4 pagesBBB Vs AAA. GR 193225 February 9, 2015docxJoeyBoyCruzNo ratings yet
- Procurement Management Plan TemplateDocument7 pagesProcurement Management Plan Templatekareem3456No ratings yet
- Main Engine Cylinder Liner Crack: Return To TOCDocument2 pagesMain Engine Cylinder Liner Crack: Return To TOCRani NoumanNo ratings yet