You might also like
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Nursing Process in Psychiatric NursingDocument14 pagesNursing Process in Psychiatric NursingJomark Palgan100% (1)
- Nursing Process in Psychiatric Unit - 3Document138 pagesNursing Process in Psychiatric Unit - 3Lina DsouzaNo ratings yet
- Community Focused Nursing: Passbooks Study GuideFrom EverandCommunity Focused Nursing: Passbooks Study GuideNo ratings yet
- The Standards of Psychiatric NursingDocument51 pagesThe Standards of Psychiatric NursingBonnie Bennet100% (1)
- Fundamentals of NursingDocument48 pagesFundamentals of Nursinganon-429003100% (31)
- MATERNAL AND CHILD HEALTH NURSE: Passbooks Study GuideFrom EverandMATERNAL AND CHILD HEALTH NURSE: Passbooks Study GuideNo ratings yet
- Psychiatric and Mental Health NursingDocument4 pagesPsychiatric and Mental Health Nursingedomilies524100% (1)
- NCM 117 - Nurse Patient Interaction - April 2021Document58 pagesNCM 117 - Nurse Patient Interaction - April 2021kimberly dedaseNo ratings yet
- Eating Disorders and Nursing CareDocument36 pagesEating Disorders and Nursing CareMuhammad Arsyad SubuNo ratings yet
- Chapter 16 SchizophreniaDocument9 pagesChapter 16 SchizophreniaCatia FernandesNo ratings yet
- Therapeutic Nurse Patient RelationshipDocument7 pagesTherapeutic Nurse Patient RelationshipPrathibha Lydia Braggs DsouzaNo ratings yet
- Basic Concepts in Psychiatric NursingDocument1,338 pagesBasic Concepts in Psychiatric Nursingdolly joy75% (4)
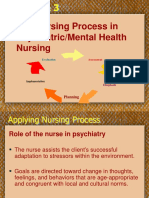
- The Nursing Process in Psychiatric/Mental Health Nursing: PlanningDocument49 pagesThe Nursing Process in Psychiatric/Mental Health Nursing: PlanningJonalynCollodChewacheo50% (2)
- Psychiatric Nursing ReviewDocument332 pagesPsychiatric Nursing Reviewkexonlagod100% (2)
- Milieu TherapyDocument4 pagesMilieu TherapyManu Sethi100% (1)
- Ethico-Legal Issues in NursingDocument34 pagesEthico-Legal Issues in NursingraghumscnNo ratings yet
- Mieliu TherapyDocument7 pagesMieliu TherapyRENJULALNo ratings yet
- Quality AssDocument57 pagesQuality AssShailja Sharma50% (2)
- Therapeutic Communication in Psychiatric NursingDocument7 pagesTherapeutic Communication in Psychiatric NursingKatrina BuenconsejoNo ratings yet
- Psychiatric Nursing 2Document14 pagesPsychiatric Nursing 2api-3731845100% (3)
- Anxiety DisordersDocument8 pagesAnxiety DisordersSydney DeringNo ratings yet
- PMH Nursing Care Plan 01112017Document19 pagesPMH Nursing Care Plan 01112017api-371817203No ratings yet
- Chapter 12 Abuse and ViolenceDocument5 pagesChapter 12 Abuse and ViolenceCatia FernandesNo ratings yet
- Documentation in Psychiatric NursingDocument15 pagesDocumentation in Psychiatric NursingShiiza Dusong Tombucon-Asis86% (7)
- Psychiatric Nursing Practice Test 1Document15 pagesPsychiatric Nursing Practice Test 1Filipino Nurses CentralNo ratings yet
- Role - Responsibilities of Psychiatry Health NurseDocument3 pagesRole - Responsibilities of Psychiatry Health NurseDhAiRyA ArOrANo ratings yet
- NCP For Adjustment DisordersDocument18 pagesNCP For Adjustment Disordersshaider119100% (1)
- Nursing Precautions For Suicidal PatientDocument6 pagesNursing Precautions For Suicidal PatientSimran JosanNo ratings yet
- Psychiatric Nursing2 Questions)Document6 pagesPsychiatric Nursing2 Questions)Pamela MagsajoNo ratings yet
- Assessment & Management of Endocrine DisordersDocument45 pagesAssessment & Management of Endocrine DisordersJerilee SoCute WattsNo ratings yet
- Community Mental Health Nursing PDFDocument2 pagesCommunity Mental Health Nursing PDFSierra67% (3)
- Anorexia vs Bulimia: Understanding Eating DisordersDocument19 pagesAnorexia vs Bulimia: Understanding Eating DisordersNylia AtibiNo ratings yet
- Chapter 3 Psychosocial Theories and TherapyDocument10 pagesChapter 3 Psychosocial Theories and TherapyCatia FernandesNo ratings yet
- Everything You Need to Know About Nursing Care PlansDocument12 pagesEverything You Need to Know About Nursing Care PlansGladys Tamayo100% (1)
- PowerPoint Presentation To Accompany Videbeck's Psychiatric Mental Health NursingDocument18 pagesPowerPoint Presentation To Accompany Videbeck's Psychiatric Mental Health NursingDennis James BartolomeNo ratings yet
- Principles of Psychiatric NursingDocument27 pagesPrinciples of Psychiatric NursingRakesh KumarNo ratings yet
- Teaching Plan - MastitisDocument2 pagesTeaching Plan - Mastitisapi-245887979No ratings yet
- Psychiatric Nursing InterventionsDocument8 pagesPsychiatric Nursing InterventionsdhodejunlNo ratings yet
- Benner's Novice to Expert Nursing TheoryDocument8 pagesBenner's Novice to Expert Nursing TheorySharwan KumawatNo ratings yet
- Pyschiatric NursingDocument40 pagesPyschiatric Nursingtheglobalnursing100% (1)
- Nursing Implementation ProcessDocument16 pagesNursing Implementation ProcessJoviNo ratings yet
- CHP 4 Patient and Caregiver Teaching StudentDocument24 pagesCHP 4 Patient and Caregiver Teaching StudentSwetaNo ratings yet
- Nursing ProcessDocument4 pagesNursing ProcessTine GuibaoNo ratings yet
- PERIOPERATIVE NURSING OVERVIEWDocument93 pagesPERIOPERATIVE NURSING OVERVIEWJoel Santos100% (1)
- Medical Surgical Nursing Review 1Document422 pagesMedical Surgical Nursing Review 1jeshemaNo ratings yet
- Maintaining Professional Boundaries in NursingDocument15 pagesMaintaining Professional Boundaries in NursingSeham Aly100% (1)
- Transcultural NursingDocument170 pagesTranscultural Nursingmirai desuNo ratings yet
- Mental Health Nursing Practice Test 1Document14 pagesMental Health Nursing Practice Test 1Dr. Jayesh Patidar100% (25)
- Nursing Care and Management of Client With SchizophreniaDocument29 pagesNursing Care and Management of Client With SchizophreniaMaizatul Akmar IbrahimNo ratings yet
- Legal psychiatric nursing issues commitment rights confidentiality negligenceDocument17 pagesLegal psychiatric nursing issues commitment rights confidentiality negligenceBrandon Arete100% (1)
- Additional Info For SchizophreniaDocument11 pagesAdditional Info For SchizophreniaJasmin JacobNo ratings yet
- Nursing Process PsychiatricDocument13 pagesNursing Process PsychiatricamitNo ratings yet
- NCM 101 - LP 1 Content PDFDocument25 pagesNCM 101 - LP 1 Content PDFDaisy RoseteNo ratings yet
- Mental Status ExaminationDocument17 pagesMental Status ExaminationRahul Khillare100% (1)
- Nursing Interventions for High Blood PressureDocument7 pagesNursing Interventions for High Blood PressureChia OliverNo ratings yet
- The Initial Psychiatric Interview PDFDocument4 pagesThe Initial Psychiatric Interview PDFJoan ChoiNo ratings yet
- 31 Therapeutic Communication Techniques With Elderly and Children2Document42 pages31 Therapeutic Communication Techniques With Elderly and Children2Ab Staholic BoiiNo ratings yet
- Internship Handbook UpdtdDocument41 pagesInternship Handbook UpdtdKalyaniGadre67% (3)
- Clinical Manual of Psychosomatic Medicine A Guide To ConsultatiDocument565 pagesClinical Manual of Psychosomatic Medicine A Guide To ConsultatiDalal HazelNo ratings yet
- Psychiatric Clerk SheetDocument7 pagesPsychiatric Clerk Sheet0045 NAZIRA ZATY BINTI ABD KARIMNo ratings yet
- Mental Status ExaminationDocument2 pagesMental Status ExaminationEna RodasNo ratings yet
- 14 - Neuropsychological AssessmentDocument14 pages14 - Neuropsychological AssessmentMARIE ROSE L. FUNTANARNo ratings yet
- How Self-Awareness and Personal Growth Can Help Overcome LimitsDocument3 pagesHow Self-Awareness and Personal Growth Can Help Overcome LimitsMelvin D. RamosNo ratings yet
- Mental Status Examination Psychiatric Nursing Assessment SpeechDocument2 pagesMental Status Examination Psychiatric Nursing Assessment SpeechElaine Louise O. Foronda100% (1)
- Mental Status Examination: Sweekaar Academy of Rehabilitation Sciences, SecunderabadDocument77 pagesMental Status Examination: Sweekaar Academy of Rehabilitation Sciences, SecunderabadSarin DominicNo ratings yet
- The Mental Status ExaminationDocument10 pagesThe Mental Status ExaminationSalvara Jane DanielNo ratings yet
- The Mental Status Examination: Dr. Ramesh Parmar Department of Psychiatry PDU Medical College, RajkotDocument33 pagesThe Mental Status Examination: Dr. Ramesh Parmar Department of Psychiatry PDU Medical College, RajkotRamashanker YadavNo ratings yet
- Case History Proforma for Psychosocial AssessmentDocument8 pagesCase History Proforma for Psychosocial AssessmentPrakash MangaloreNo ratings yet
- DHF2 CasepediaDocument2 pagesDHF2 CasepediaKen ZaireNo ratings yet
- Behavioral Health NeurpsycatricDocument297 pagesBehavioral Health NeurpsycatricRohit SagarNo ratings yet
- Outline of Mental Status ExaminationDocument10 pagesOutline of Mental Status ExaminationMohammed Hosen100% (1)
- Midterm ExamDocument29 pagesMidterm ExamCharissa de LeonNo ratings yet
- UoHpsychjr OSCE 2021Document19 pagesUoHpsychjr OSCE 2021sakariyeNo ratings yet
- Final Answer Key for Occupational Therapist ExamDocument11 pagesFinal Answer Key for Occupational Therapist Examdeepanshi vashishtha100% (1)
- Study Guide Behavior Semester IV FK UNUDDocument67 pagesStudy Guide Behavior Semester IV FK UNUDPadma PermanaNo ratings yet
- Process RecordingDocument3 pagesProcess Recordingapi-353044299100% (4)
- MSE Sample PDFDocument5 pagesMSE Sample PDFSam Raven AndresNo ratings yet
- Lezak. Neuropsychological Assessment (5th Edition)Document1,576 pagesLezak. Neuropsychological Assessment (5th Edition)Anneliese Fuentes95% (107)
- Vii. General Survey: Gerontologic Nursing 6th Edition, Meiner S. & Yeager J., P. 37Document2 pagesVii. General Survey: Gerontologic Nursing 6th Edition, Meiner S. & Yeager J., P. 37AvyNo ratings yet
- Daily Nursing AssessmentDocument2 pagesDaily Nursing Assessmentkiku_laiNo ratings yet
- Vol 24.3 - Behavioral Neurology and Psychiatry.2018Document343 pagesVol 24.3 - Behavioral Neurology and Psychiatry.2018Tatiana Patricia Cantillo FadulNo ratings yet
- VSIM Bipolar Disorder Sharon ColeDocument3 pagesVSIM Bipolar Disorder Sharon Cole002100% (1)
- Form 1 QuestionsDocument12 pagesForm 1 Questionsshahid100% (4)
- CH30Document89 pagesCH30Jan Oliver YaresNo ratings yet
- Get Through Workplace Based Assessments in PsychiatryDocument200 pagesGet Through Workplace Based Assessments in Psychiatrysherief marouf100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (31)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)