You might also like
- Pharmacology AntibioticsDocument70 pagesPharmacology Antibioticsmaggie100% (1)
- Why Are Black Women Rated Less Physically Attractive Than Other Women, But Black Men Are Rated Better Looking Than Other Men?Document6 pagesWhy Are Black Women Rated Less Physically Attractive Than Other Women, But Black Men Are Rated Better Looking Than Other Men?koa_x100% (2)
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Crisis CounsellingDocument28 pagesCrisis CounsellingPooja varmaNo ratings yet
- NCP For DMDocument14 pagesNCP For DMLynzzky Virtudes AbranNo ratings yet
- The Role of A Pastor As A CounselorDocument5 pagesThe Role of A Pastor As A Counselorkhetsiwe gule100% (2)
- Generic Name Brand Names Common Uses Possible Side Effects Mechanism of ActionDocument13 pagesGeneric Name Brand Names Common Uses Possible Side Effects Mechanism of Actionangel3424No ratings yet
- EssayDocument2 pagesEssayFelipe AndinoNo ratings yet
- Nebulization: Presented By: Ms. Sinsu Rachel Alex Msc. (N) Prev YrDocument29 pagesNebulization: Presented By: Ms. Sinsu Rachel Alex Msc. (N) Prev Yrmanoj reddy100% (1)
- First Steps in REBT - Windy DrydenDocument44 pagesFirst Steps in REBT - Windy DrydenStefan Alexandru100% (4)
- A Case Study On SchizophreniaDocument11 pagesA Case Study On SchizophreniaRosa Isabel57% (7)
- Pharmacology - Chapter 29Document5 pagesPharmacology - Chapter 29Ashley-Michelle LewisNo ratings yet
- Emergency Department Handbook PDFDocument461 pagesEmergency Department Handbook PDFdmallozziNo ratings yet
- Obstetric Analgesia PDFDocument45 pagesObstetric Analgesia PDFBoneyJalgar100% (1)
- List of AntibioticsDocument11 pagesList of AntibioticsD. BarNo ratings yet
- I-STAT Hospital Navigator BrochureDocument19 pagesI-STAT Hospital Navigator BrochureClaudia SotoNo ratings yet
- CeftazidimeDocument16 pagesCeftazidimeNakorn BaisriNo ratings yet
- CARBAPENEMSDocument87 pagesCARBAPENEMSvijayabhavani.sNo ratings yet
- Faces Iv and The Circumplex Model - Validation Study PDFDocument17 pagesFaces Iv and The Circumplex Model - Validation Study PDFjulinau25No ratings yet
- OFRAMAX 250 (Injection) OFRAMAX 1 G (Injection)Document4 pagesOFRAMAX 250 (Injection) OFRAMAX 1 G (Injection)mahgadNo ratings yet
- Ceftomax S InjDocument9 pagesCeftomax S InjIjlal GhaniNo ratings yet
- Claforan (Cefotaxime) PDFDocument18 pagesClaforan (Cefotaxime) PDFdinniNo ratings yet
- Cefotaxime: Cefotaxime (Cefotaxime For Injection) For Injection USP and Dextrose InjectionDocument21 pagesCefotaxime: Cefotaxime (Cefotaxime For Injection) For Injection USP and Dextrose InjectionYaleswari Hayu PertiwiNo ratings yet
- Management of Uncomplicated Urinary Tract InfectionDocument38 pagesManagement of Uncomplicated Urinary Tract Infectionhuddy101No ratings yet
- Tetracyclines: Mechanism of ActionDocument16 pagesTetracyclines: Mechanism of Actionammar amerNo ratings yet
- CefaclorsandozcapDocument9 pagesCefaclorsandozcapseagull70No ratings yet
- Cephalosporins, Flouroquinolones and SulfonamidesDocument7 pagesCephalosporins, Flouroquinolones and SulfonamidesErum JanNo ratings yet
- 31Document4 pages31Noman AliNo ratings yet
- MoxifloxacinDocument3 pagesMoxifloxacinWaseem HaiderNo ratings yet
- MIC CefadroxilDocument14 pagesMIC CefadroxilanggiNo ratings yet
- Drugs PocDocument2 pagesDrugs PocJean SandoyNo ratings yet
- CefaclorDocument3 pagesCefaclorAyah PaasaNo ratings yet
- Ceftriaxoneinj DEVADocument11 pagesCeftriaxoneinj DEVAMuhammad AwaisNo ratings yet
- Blunt Abdominal Trauma MedicationDocument8 pagesBlunt Abdominal Trauma MedicationYudis Wira PratamaNo ratings yet
- 20120424Document17 pages20120424Afsal Ur FriendNo ratings yet
- NETSPAN Injection (Netilmicin Sulfate) : CompositionDocument9 pagesNETSPAN Injection (Netilmicin Sulfate) : CompositionIntan Rizqi RahmawatiNo ratings yet
- Profort VialDocument8 pagesProfort Vialelcapitano vegetaNo ratings yet
- Antibiotics 11.05.19Document18 pagesAntibiotics 11.05.19dahiphale1No ratings yet
- Overview of AntibioticsDocument5 pagesOverview of AntibioticsakshahinbdNo ratings yet
- Pharma Uro Cotrimoxazole +fqsDocument14 pagesPharma Uro Cotrimoxazole +fqsHussein AlhaddadNo ratings yet
- Cefoperazone and SulbactumDocument3 pagesCefoperazone and Sulbactumiloveit52252No ratings yet
- Nursing 3703 Pharmacology: Antimicrobials by Linda SelfDocument78 pagesNursing 3703 Pharmacology: Antimicrobials by Linda Selfdon yenNo ratings yet
- Cefazolin (Ancef ®) : D5W, NsDocument9 pagesCefazolin (Ancef ®) : D5W, Nsbabe5606No ratings yet
- List of Antibiotics: Following Is The List Of, Sorted by Class. The Highest Division Is BetweenDocument11 pagesList of Antibiotics: Following Is The List Of, Sorted by Class. The Highest Division Is BetweenBhanuprakash PuthalapattuNo ratings yet
- Leflocad 500 MGDocument39 pagesLeflocad 500 MGamr ahmedNo ratings yet
- 1.3.1.1 Ireland Tavanic 500mg SMPC PDFDocument19 pages1.3.1.1 Ireland Tavanic 500mg SMPC PDFНатали КапанадзеNo ratings yet
- PharmaDocument16 pagesPharmaPaula Grace MorfeNo ratings yet
- Chloramphenicol: Ayen University - Al College of PharmacyDocument7 pagesChloramphenicol: Ayen University - Al College of Pharmacyمحمد حميد عطيةNo ratings yet
- Aus Pi TargocidDocument5 pagesAus Pi TargocidAsto Ata InteristiNo ratings yet
- Las 7 PcolDocument47 pagesLas 7 Pcoljenet soleilNo ratings yet
- Floxel 148Document1 pageFloxel 148scribd scribdNo ratings yet
- Pharma URO AminoglycosidesDocument8 pagesPharma URO AminoglycosidesHussein AlhaddadNo ratings yet
- En Web Insert Cefaz NLDocument3 pagesEn Web Insert Cefaz NLAbdul AzizNo ratings yet
- MoxicipDocument12 pagesMoxicipSiva LakshmiNarayananNo ratings yet
- COTRIMOXAZOLE +FQsDocument62 pagesCOTRIMOXAZOLE +FQsHussein AlhaddadNo ratings yet
- Staphylococcus Saprophyticus in As Many As 5% To 15% of Cases. Enterococci, Klebsiella Species and Proteus Mirabilis Account For A Small Percentage of Overall InfectionsDocument6 pagesStaphylococcus Saprophyticus in As Many As 5% To 15% of Cases. Enterococci, Klebsiella Species and Proteus Mirabilis Account For A Small Percentage of Overall InfectionsMarzina AjrinNo ratings yet
- Ceftriaxone Monograph - PaediatricDocument6 pagesCeftriaxone Monograph - PaediatricGheorghe Stefan-SorinNo ratings yet
- List of AntibioticsDocument10 pagesList of AntibioticsAia JavierNo ratings yet
- Pharmacology of Antiparasit DrugsDocument40 pagesPharmacology of Antiparasit Drugsakun scribNo ratings yet
- CEFACLOR-cefaclor Caps Ule Carls Bad Technology, IncDocument13 pagesCEFACLOR-cefaclor Caps Ule Carls Bad Technology, IncsadafNo ratings yet
- Antibiotik Dan Antiseptik Saluran KemihDocument29 pagesAntibiotik Dan Antiseptik Saluran KemihPutri Sari SeptirianiNo ratings yet
- CeftriaxoneaftinjDocument18 pagesCeftriaxoneaftinjbarbawurakNo ratings yet
- Commonly Used Veterinary Drugs in VTH, SPANA, DONKEY SANCTUARYDocument36 pagesCommonly Used Veterinary Drugs in VTH, SPANA, DONKEY SANCTUARYyomifNo ratings yet
- Cefprozil Final ProductDocument18 pagesCefprozil Final ProductRathnaganpathi ThulasikumarNo ratings yet
- CephalosporinDocument34 pagesCephalosporinliamhenry9449No ratings yet
- Cefuroxime PM ENG v6.0 052820Document33 pagesCefuroxime PM ENG v6.0 052820dhanrajsen12121990No ratings yet
- List of Antibiotics - Wikipedia, The Free EncyclopediaDocument11 pagesList of Antibiotics - Wikipedia, The Free EncyclopediaRamesh KumarNo ratings yet
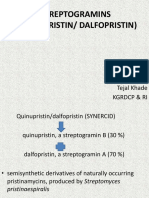
- Streptogramins (Quinupristin/ Dalfopristin) : Tejal Khade KGRDCP & RiDocument16 pagesStreptogramins (Quinupristin/ Dalfopristin) : Tejal Khade KGRDCP & RiAkshada bhangreNo ratings yet
- List of AntibioticsDocument9 pagesList of Antibioticsdesi_mNo ratings yet
- IpsaDocument19 pagesIpsaLuisa LopezNo ratings yet
- The Essential Guide to Ciprofloxacin: Usage, Precautions, Interactions and Side Effects.From EverandThe Essential Guide to Ciprofloxacin: Usage, Precautions, Interactions and Side Effects.No ratings yet
- Sixth ScheduleDocument3 pagesSixth Scheduleangelene koidNo ratings yet
- Art Therapy APADocument10 pagesArt Therapy APAhashmiaqeedat5No ratings yet
- Chapter 102: Laryngeal Trauma From Intubation: Endoscopic Evaluation and Classification Bruce BenjaminDocument16 pagesChapter 102: Laryngeal Trauma From Intubation: Endoscopic Evaluation and Classification Bruce BenjaminPrisia AnantamaNo ratings yet
- Medical Device PackagingDocument17 pagesMedical Device Packaging049 Nishigandha NadavadeNo ratings yet
- Internet Gaming Disorder: A Case ReportDocument4 pagesInternet Gaming Disorder: A Case ReportJAVED ATHER SIDDIQUINo ratings yet
- Cancer (Medical Term:Malignant NeoplasmDocument7 pagesCancer (Medical Term:Malignant NeoplasmolussojiNo ratings yet
- Comprehensive Assessment Diagnosis and Treatment Planning of Severe Periodontal DiseaseDocument9 pagesComprehensive Assessment Diagnosis and Treatment Planning of Severe Periodontal DiseaseJOHAYMEN MANGORSINo ratings yet
- Topical AntifungalsDocument14 pagesTopical AntifungalsRasha Mohammad100% (1)
- Bladder Calculus Resulting From The Migration of An IntrauterineDocument8 pagesBladder Calculus Resulting From The Migration of An IntrauterineFabrien Hein WillemNo ratings yet
- Strength and Conditioning Coach or Sports Performance Coach or FDocument3 pagesStrength and Conditioning Coach or Sports Performance Coach or Fapi-121340325No ratings yet
- Malaprabha Biogas Plant Developed by DR S V MapuskarDocument40 pagesMalaprabha Biogas Plant Developed by DR S V Mapuskarsvmapuskar4914100% (3)
- Leptospirosis CaseDocument29 pagesLeptospirosis CaseJp RectraNo ratings yet
- BMJ j3887 FullDocument10 pagesBMJ j3887 FullRiri Maisytoh PutriNo ratings yet
- Nursing Care For Patients With LungDocument14 pagesNursing Care For Patients With LungAyu RahayuniNo ratings yet
- Case Study Sa Surgical WardDocument8 pagesCase Study Sa Surgical WardAiza ToledanaNo ratings yet
- Hiv AidS ATSDocument65 pagesHiv AidS ATSAnton Prio WahyudiNo ratings yet
- Engineering A Healthy Body: Career CatalystDocument6 pagesEngineering A Healthy Body: Career CatalystB6D4N0No ratings yet
- Front Back: Adacium Rapid 50mg TabletsDocument1 pageFront Back: Adacium Rapid 50mg TabletsAmri MuharamNo ratings yet