You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Seven Pillars of WisdomDocument16 pagesSeven Pillars of WisdomJames100% (1)
- A Guide To Improving Data Integrity and AdoptionDocument39 pagesA Guide To Improving Data Integrity and AdoptionKevin PNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Preparation Book For The Testas Humanities Cultural Social Sciences ModuleDocument215 pagesPreparation Book For The Testas Humanities Cultural Social Sciences ModuleNapi Opil100% (1)
- 35 Dimensions of Critical ThinkngDocument13 pages35 Dimensions of Critical Thinkngapi-276941568No ratings yet
- Edexcel IGCSE 9-1 EAM Marking Scheme For Paper 1Document17 pagesEdexcel IGCSE 9-1 EAM Marking Scheme For Paper 1hussain azizNo ratings yet
- IC - Student Hat ChecksheetDocument16 pagesIC - Student Hat ChecksheetNicholas Edward Werner-MatavkaNo ratings yet
- Personal Epistemology Research: Implications For Learning and TeachingDocument31 pagesPersonal Epistemology Research: Implications For Learning and TeachingespalditoNo ratings yet
- Measuring Helix Angle of GearsDocument6 pagesMeasuring Helix Angle of Gearsdarshan.hegdebNo ratings yet
- 9225 International Gcse Business Mark Scheme 2 v1.0Document23 pages9225 International Gcse Business Mark Scheme 2 v1.0Kenny KwokNo ratings yet
- Clash of Cultural Values in Song of LawinoDocument3 pagesClash of Cultural Values in Song of Lawinodavidovulcan100% (2)
- Monument of Myth: The Basilica of Sacre CouerDocument20 pagesMonument of Myth: The Basilica of Sacre CouerGeneric_PersonaNo ratings yet
- Crown & Baptist Streets Village Group: ST Re EtDocument1 pageCrown & Baptist Streets Village Group: ST Re EtGeneric_PersonaNo ratings yet
- The Rise of The Individual in Modern ChinaDocument3 pagesThe Rise of The Individual in Modern ChinaGeneric_PersonaNo ratings yet
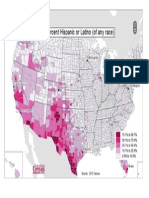
- US Map of Hispanic Population by CountyDocument1 pageUS Map of Hispanic Population by CountyGeneric_PersonaNo ratings yet
- Earnings of ImmigrantsDocument23 pagesEarnings of ImmigrantsGeneric_PersonaNo ratings yet
- Sydney As A Global CityDocument9 pagesSydney As A Global CityGeneric_PersonaNo ratings yet
- Peach Leaf CurlDocument3 pagesPeach Leaf CurlGeneric_PersonaNo ratings yet
- Citizens United ReviewDocument5 pagesCitizens United ReviewGeneric_PersonaNo ratings yet
- English Language in Hong KongDocument13 pagesEnglish Language in Hong KongGeneric_PersonaNo ratings yet
- Result of Portrayals of Latinos On TVDocument33 pagesResult of Portrayals of Latinos On TVGeneric_PersonaNo ratings yet
- Sydney Australia's Green Sector OpportunityDocument8 pagesSydney Australia's Green Sector OpportunityGeneric_PersonaNo ratings yet
- China and Sydney Australias Growing Business PartnershipDocument8 pagesChina and Sydney Australias Growing Business PartnershipGeneric_PersonaNo ratings yet
- Risk-Managing Revolution (Arab Spring)Document4 pagesRisk-Managing Revolution (Arab Spring)Generic_PersonaNo ratings yet
- Educated Preferences: Explaining Attitudes Toward Immigration in EuropeDocument44 pagesEducated Preferences: Explaining Attitudes Toward Immigration in EuropeGeneric_PersonaNo ratings yet
- The Diversity of Debt Crises in EuropeDocument18 pagesThe Diversity of Debt Crises in EuropeGeneric_PersonaNo ratings yet
- Internet, Mass Communication & Collective ActionDocument12 pagesInternet, Mass Communication & Collective ActionGeneric_PersonaNo ratings yet
- Agenda Setting, Public Opinion & Immigration ReformDocument21 pagesAgenda Setting, Public Opinion & Immigration ReformGeneric_PersonaNo ratings yet
- Empowering Youth - Technology in Advocacy To Affect Social ChangeDocument18 pagesEmpowering Youth - Technology in Advocacy To Affect Social ChangeGeneric_PersonaNo ratings yet
- Promoting Economic Liberalization in EgyptDocument14 pagesPromoting Economic Liberalization in EgyptGeneric_PersonaNo ratings yet
- Grizzly Hevy Duty Wood Lathe ManualDocument60 pagesGrizzly Hevy Duty Wood Lathe ManualGeneric_PersonaNo ratings yet
- The Rise of The Individual in Modern ChinaDocument3 pagesThe Rise of The Individual in Modern ChinaGeneric_PersonaNo ratings yet
- Prilleltensky.2008.Role of Power in Wellness-Oppression-Liberation - JCP PDFDocument21 pagesPrilleltensky.2008.Role of Power in Wellness-Oppression-Liberation - JCP PDFcastrolaNo ratings yet
- Protests in An Information SocietyDocument25 pagesProtests in An Information SocietyGeneric_PersonaNo ratings yet
- US Policy and The International Dimensions of Failed Democratic Transitions in The Arab WorldDocument18 pagesUS Policy and The International Dimensions of Failed Democratic Transitions in The Arab WorldGeneric_PersonaNo ratings yet
- A Study On The Effects of Sexually Explicit Advertisement On MemoryDocument10 pagesA Study On The Effects of Sexually Explicit Advertisement On MemoryGeneric_PersonaNo ratings yet
- English Language in Hong KongDocument13 pagesEnglish Language in Hong KongGeneric_PersonaNo ratings yet
- Hypothalamic Astrocytoma: Hyperphagia Syndrome & Accompanying IssuesDocument4 pagesHypothalamic Astrocytoma: Hyperphagia Syndrome & Accompanying IssuesGeneric_PersonaNo ratings yet
- Title Insert (Derogatory Words) Research StudyDocument5 pagesTitle Insert (Derogatory Words) Research StudyGeneric_PersonaNo ratings yet
- Aggressive Behavior Following StrokeDocument5 pagesAggressive Behavior Following StrokeGeneric_PersonaNo ratings yet
- Level 7 Assessment Specification: Appendix Ga36DDocument9 pagesLevel 7 Assessment Specification: Appendix Ga36DKanchana PereraNo ratings yet
- SENZERE A: THE HUNTER ANSWERING TECHNIQUESDocument4 pagesSENZERE A: THE HUNTER ANSWERING TECHNIQUESPro NdebeleNo ratings yet
- Assignment SE - 2017 - 022Document6 pagesAssignment SE - 2017 - 022JOSIAH PRATHABANNo ratings yet
- Using The Contextual Model of LearninDocument35 pagesUsing The Contextual Model of LearninBrenda Loiacono CabralNo ratings yet
- Use of English PDFDocument109 pagesUse of English PDFmuyi kunleNo ratings yet
- Honors Biology Quarterly Portfolio 100-120 PointsDocument2 pagesHonors Biology Quarterly Portfolio 100-120 Pointsanon_865386332No ratings yet
- 03 Positive and Negative Effects of ReligionDocument15 pages03 Positive and Negative Effects of ReligionRay Hope P PuracanNo ratings yet
- Solution of UHV Paper CT 1 2021-2022Document11 pagesSolution of UHV Paper CT 1 2021-2022PiyushNo ratings yet
- Vibration MeterDocument11 pagesVibration MeterNatNo ratings yet
- Cambridge O Level: Setswana 3158/02 October/November 2020Document21 pagesCambridge O Level: Setswana 3158/02 October/November 2020Segomotso MbaiwaNo ratings yet
- Mathematics Mastery Year 4 Unit 1 Guide 1 PDFDocument5 pagesMathematics Mastery Year 4 Unit 1 Guide 1 PDFNur Bahar YeashaNo ratings yet
- Instructional Plan IPlan TemplateDocument7 pagesInstructional Plan IPlan TemplateIT AguilarNo ratings yet
- BIS2003 Assessment Brief T2 2022-2Document9 pagesBIS2003 Assessment Brief T2 2022-2usmanNo ratings yet
- QUARTER-1-EFDT - MATH 10 Learning-PlanDocument11 pagesQUARTER-1-EFDT - MATH 10 Learning-PlanFaculty SFANo ratings yet
- A Practical Guide To Academic ExcellenceDocument57 pagesA Practical Guide To Academic ExcellenceWallace MonibidorNo ratings yet
- Coursework 2 - Brief and Guidance 2018-19Document12 pagesCoursework 2 - Brief and Guidance 2018-19Hans HoNo ratings yet
- General Math FullDocument8 pagesGeneral Math FullWnc WestridgeNo ratings yet
- As Film Studies Coursework Storyboard IdeasDocument1 pageAs Film Studies Coursework Storyboard Ideasafaydoter100% (2)
- Owen Gates 18354629 - Tpa Report Minimum SizeDocument92 pagesOwen Gates 18354629 - Tpa Report Minimum Sizeapi-554394021No ratings yet
- Crossing Over: Introducing The Threshold Project. 2013 Strengthening Student Success ConferenceDocument27 pagesCrossing Over: Introducing The Threshold Project. 2013 Strengthening Student Success Conference3CSNNo ratings yet
- Bennys Pennies Lesson PlanDocument3 pagesBennys Pennies Lesson Planapi-253597352No ratings yet