You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ciolli G ArberDocument41 pagesCiolli G ArberAirB13No ratings yet
- Elementary English Review 4 Units 28 35 British English StudentDocument8 pagesElementary English Review 4 Units 28 35 British English StudentSamuel RuibascikiNo ratings yet
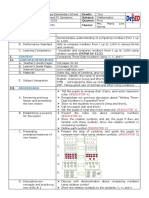
- Mathematics1 Hiligaynon Daily Lesson Log Q1W1Document5 pagesMathematics1 Hiligaynon Daily Lesson Log Q1W1Maria Theresa VillaruzNo ratings yet
- IITH Staff Recruitment NF 9 Detailed Advertisement 11-09-2021Document14 pagesIITH Staff Recruitment NF 9 Detailed Advertisement 11-09-2021junglee fellowNo ratings yet
- Textbook of Oral Medicine Oral DiagnosisDocument924 pagesTextbook of Oral Medicine Oral DiagnosisSonal100% (1)
- Comparing Numbers (2021 - 06 - 19 01 - 35 - 12 UTC) (2021 - 08 - 06 04 - 51 - 25 UTC)Document3 pagesComparing Numbers (2021 - 06 - 19 01 - 35 - 12 UTC) (2021 - 08 - 06 04 - 51 - 25 UTC)ALLinOne BlogNo ratings yet
- Attendance Monitoring System and Information Dissemination With Sms Dissemination"Document4 pagesAttendance Monitoring System and Information Dissemination With Sms Dissemination"Emmanuel Baccaray100% (1)
- Film Scene Comparison Essay PromptDocument2 pagesFilm Scene Comparison Essay PromptScarlett PackNo ratings yet
- Facilitator PDFDocument8 pagesFacilitator PDFAnand ChoubeyNo ratings yet
- Full Text of The Official Result of The April 2014 Librarian Licensure ExaminationDocument2 pagesFull Text of The Official Result of The April 2014 Librarian Licensure ExaminationnasenagunNo ratings yet
- Design Thinking A Guide To Creative Problem Solving For Everyone PDFDocument177 pagesDesign Thinking A Guide To Creative Problem Solving For Everyone PDFCarmen Saborio100% (5)
- FreeLandformsBulletinBoardPostersandMatchingActivity PDFDocument28 pagesFreeLandformsBulletinBoardPostersandMatchingActivity PDFDharani JagadeeshNo ratings yet
- Toronto Public Library - Circulation and Collection Use (Including Fees Andfines) Policy - 2013 RecommendationsDocument10 pagesToronto Public Library - Circulation and Collection Use (Including Fees Andfines) Policy - 2013 RecommendationsLJ's infoDOCKETNo ratings yet
- 5 e Model Science Lesson Plan TemplateDocument4 pages5 e Model Science Lesson Plan TemplateMaestro UseroNo ratings yet
- AssessmentDocument9 pagesAssessmentJohn AndrewNo ratings yet
- Music Min Workshop PDFDocument15 pagesMusic Min Workshop PDFKent Cena RamosNo ratings yet
- 5e Lesson-AmharveyDocument3 pages5e Lesson-Amharveyapi-352123670100% (1)
- Gujarat Cbse SchoolDocument47 pagesGujarat Cbse Schoolramansharma1769No ratings yet
- Panjab University BA SyllabusDocument245 pagesPanjab University BA SyllabusAditya SharmaNo ratings yet
- 師伝芥考土佐の英信流Document71 pages師伝芥考土佐の英信流任平生No ratings yet
- Self Hypnosis: Hypnosis and The Unconscious MindDocument6 pagesSelf Hypnosis: Hypnosis and The Unconscious MindSai BhaskarNo ratings yet
- Lifespan Development 7th Edition Boyd Test BankDocument31 pagesLifespan Development 7th Edition Boyd Test Bankbrandoncoletjaxprigfm100% (32)
- Basic Research DesignsDocument5 pagesBasic Research DesignsKaia LouisNo ratings yet
- Lesson X Selecting Instructional MaterialsDocument18 pagesLesson X Selecting Instructional MaterialsLarah Joy BasitNo ratings yet
- Synopsis OSCEDocument5 pagesSynopsis OSCEPrasann RoyNo ratings yet
- How To Answer Bi Paper 1 and Paper 2 Wisely and Effectively by PDocument21 pagesHow To Answer Bi Paper 1 and Paper 2 Wisely and Effectively by PNorlida Abd RahmanNo ratings yet
- A Study On Customer Satisfaction Towards " Asian Paints" (With Reference To Hightech Paint Shopee, Adoni)Document7 pagesA Study On Customer Satisfaction Towards " Asian Paints" (With Reference To Hightech Paint Shopee, Adoni)RameshNo ratings yet
- Seva Bharathi Kishori Vikas - EnglishDocument15 pagesSeva Bharathi Kishori Vikas - EnglishSevaBharathiTelanganaNo ratings yet
- CST 47 TeacherDocument56 pagesCST 47 TeacherElena DavalosNo ratings yet
- Asafa Book Oromuma PDFDocument183 pagesAsafa Book Oromuma PDFgemechuNo ratings yet