You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- MCPS Sports Concussion Data 2014-15Document1 pageMCPS Sports Concussion Data 2014-15Concussion_MCPS_MdNo ratings yet
- Parent Letter To MCPS Re Student Injury Data - 01-14-2015Document11 pagesParent Letter To MCPS Re Student Injury Data - 01-14-2015Concussion_MCPS_MdNo ratings yet
- NFL 2010 Letter Re Concussion LegDocument2 pagesNFL 2010 Letter Re Concussion LegConcussion_MCPS_MdNo ratings yet
- MCPS (MD) Tobacco-Free SCH PolicyDocument2 pagesMCPS (MD) Tobacco-Free SCH PolicyConcussion_MCPS_MdNo ratings yet
- Brain Sentry Inova Football Helmet Sensor Research Study ProposalDocument5 pagesBrain Sentry Inova Football Helmet Sensor Research Study ProposalConcussion_MCPS_MdNo ratings yet
- Template 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Document1 pageTemplate 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Concussion_MCPS_MdNo ratings yet
- MCPS Student Injury Report FormDocument2 pagesMCPS Student Injury Report FormConcussion_MCPS_MdNo ratings yet
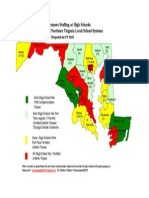
- Projected Ath Trainer HS Staffing in FY 2015-Map of MD and N. VA CountiesDocument1 pageProjected Ath Trainer HS Staffing in FY 2015-Map of MD and N. VA CountiesConcussion_MCPS_MdNo ratings yet
- MD Bill - HS Football Helmet Sensor Pilot ProgramDocument6 pagesMD Bill - HS Football Helmet Sensor Pilot ProgramConcussion_MCPS_MdNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chest DrainageDocument22 pagesChest DrainageAmeliaM100% (7)
- Title/Details Provider CEU: NSCA CEU Approved Home Study ActivitiesDocument38 pagesTitle/Details Provider CEU: NSCA CEU Approved Home Study ActivitiesPeter WalidNo ratings yet
- Tom Myers 10 Tips For Fascial FitnessDocument11 pagesTom Myers 10 Tips For Fascial Fitnessspiraldao100% (6)
- FENO As Monitoring Tool in Bronchial Asthma A Randomised Control TrialDocument23 pagesFENO As Monitoring Tool in Bronchial Asthma A Randomised Control TrialYadvir GargNo ratings yet
- Individual Adlerian Psychology CounselingDocument5 pagesIndividual Adlerian Psychology CounselinghopeIshanzaNo ratings yet
- Brosur Bubble CPAP Pigeon BaruDocument2 pagesBrosur Bubble CPAP Pigeon Baruteguh nugrohoNo ratings yet
- Lumie Vitamin L User ManualDocument56 pagesLumie Vitamin L User ManualsighsighsighNo ratings yet
- Published Books by ERDODocument19 pagesPublished Books by ERDODebasish KunduNo ratings yet
- MEDraysintell Nuclear Medicine Edition 2017 - Summary and TOCDocument6 pagesMEDraysintell Nuclear Medicine Edition 2017 - Summary and TOCLadipo Temitope AyodejiNo ratings yet
- Breast Cancer ProtocolDocument24 pagesBreast Cancer Protocolsilveo100% (1)
- 13 EMT Airway Management Slides PDFDocument51 pages13 EMT Airway Management Slides PDFDhimas Bimantara100% (1)
- NBME 1 Block 1 - 4 EditedDocument77 pagesNBME 1 Block 1 - 4 Editedalex karevNo ratings yet
- Secondary Arterial HypertensionDocument32 pagesSecondary Arterial HypertensionAndi SusiloNo ratings yet
- Assessment of Knowledge of Public On Coronary Artery Disease, Hypertension and Diabetes MellitusDocument5 pagesAssessment of Knowledge of Public On Coronary Artery Disease, Hypertension and Diabetes MellitusMythili MuthappaNo ratings yet
- CvHeel Revisiting BoyesenDocument33 pagesCvHeel Revisiting BoyesenEscarro100% (1)
- Pharmacological Management of Type 1 DiabetesDocument6 pagesPharmacological Management of Type 1 DiabetesMI RFNo ratings yet
- Preeclampsia Diagnosis and Treatment OptionsDocument14 pagesPreeclampsia Diagnosis and Treatment OptionsPanji Agung KhrisnaNo ratings yet
- DMSCO Log Book Vol.13 1936Document49 pagesDMSCO Log Book Vol.13 1936Des Moines University Archives and Rare Book RoomNo ratings yet
- Mixed Dentition Ortho Treatment / Orthodontic Courses by Indian Dental AcademyDocument116 pagesMixed Dentition Ortho Treatment / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Research2 1Document4 pagesResearch2 1mohamadrenegadeNo ratings yet
- Work Setting of CounselorDocument3 pagesWork Setting of CounselorAngel Rose Sierda MedinaNo ratings yet
- Nutrition For Patients With in ThalassemiaDocument27 pagesNutrition For Patients With in ThalassemiaSalaudeen IlyasNo ratings yet
- New Clinical Analysis and Device For Botox InjectionsDocument4 pagesNew Clinical Analysis and Device For Botox Injectionsleenatalia93No ratings yet
- Lumbal PunctureDocument2 pagesLumbal PunctureAkbarsyah Ridar AditamaNo ratings yet
- Cerebral PalsyDocument97 pagesCerebral PalsyPrernaSharma100% (3)
- Carti DermatoDocument29 pagesCarti Dermatosepis10No ratings yet
- Malaria Treatment 2013Document75 pagesMalaria Treatment 2013Rheinny IndrieNo ratings yet
- The Efficacy of Psychodynamic Psychotherapy Jonathan Shedler PDFDocument12 pagesThe Efficacy of Psychodynamic Psychotherapy Jonathan Shedler PDFManuel PernetasNo ratings yet
- Moringa Cure Fever PDFDocument4 pagesMoringa Cure Fever PDFCisco SilvaNo ratings yet
- Aromatase InhibitorDocument10 pagesAromatase InhibitorBenny KurniawanNo ratings yet