You might also like
- Guidelines For The Management of Adult Acute and Acute-on-Chronic Liver Failure in The ICUDocument3 pagesGuidelines For The Management of Adult Acute and Acute-on-Chronic Liver Failure in The ICUkrisna129No ratings yet
- ECG-Guided Localization of RVOT and LVOT ArrhythmiasDocument46 pagesECG-Guided Localization of RVOT and LVOT Arrhythmiaskrisna129No ratings yet
- CARDIO PDF Presentation 2 PDFDocument11 pagesCARDIO PDF Presentation 2 PDFAlexis Camille SanidadNo ratings yet
- Munson-Tucker1975 Article DosesOfEpinephrineCausingArrhy PDFDocument7 pagesMunson-Tucker1975 Article DosesOfEpinephrineCausingArrhy PDFkrisna129No ratings yet
- Regional Versus General Anesthesia in Surgical Patients With Chronic Obstructive Pulmonary Disease: Does Avoiding General Anesthesia Reduce The Risk of Postoperative Complications?Document8 pagesRegional Versus General Anesthesia in Surgical Patients With Chronic Obstructive Pulmonary Disease: Does Avoiding General Anesthesia Reduce The Risk of Postoperative Complications?mluthfidunandNo ratings yet
- Munson-Tucker1975 Article DosesOfEpinephrineCausingArrhy PDFDocument7 pagesMunson-Tucker1975 Article DosesOfEpinephrineCausingArrhy PDFkrisna129No ratings yet
- Regional Versus General Anesthesia in Surgical Patients With Chronic Obstructive Pulmonary Disease: Does Avoiding General Anesthesia Reduce The Risk of Postoperative Complications?Document8 pagesRegional Versus General Anesthesia in Surgical Patients With Chronic Obstructive Pulmonary Disease: Does Avoiding General Anesthesia Reduce The Risk of Postoperative Complications?mluthfidunandNo ratings yet
- Usefullnes of QT Interval PDFDocument14 pagesUsefullnes of QT Interval PDFkrisna129No ratings yet
- 133 FullDocument3 pages133 Fullkrisna129No ratings yet
- Transkrip Nilai 2 PDFDocument1 pageTranskrip Nilai 2 PDFkrisna129No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Drug Study - TramadolDocument1 pageDrug Study - TramadolLeslie LibrandoNo ratings yet
- PHYCHOSOCIAL INTEGRITY EditedDocument122 pagesPHYCHOSOCIAL INTEGRITY EditedjasonNo ratings yet
- Review of Drugs Evidence Pack - FINAL PUBLICATION VERSION 1Document125 pagesReview of Drugs Evidence Pack - FINAL PUBLICATION VERSION 1Colin Moore100% (1)
- Antidote Meds in Crash Cart (Naloxone, Hydrobromide, Flumazenil)Document5 pagesAntidote Meds in Crash Cart (Naloxone, Hydrobromide, Flumazenil)Still DollNo ratings yet
- Pharmacology On Your PalmsDocument75 pagesPharmacology On Your PalmsReza JahanimirNo ratings yet
- 10 MRCP 2 Oncology NOTES Passmedicine PDFDocument54 pages10 MRCP 2 Oncology NOTES Passmedicine PDFHussein GhannamNo ratings yet
- From Pioneer Days To Implementation - Lessons To Be LearntDocument5 pagesFrom Pioneer Days To Implementation - Lessons To Be LearntThiago GomesNo ratings yet
- Decision Making in Pain ManagementDocument319 pagesDecision Making in Pain Managementabdul100% (1)
- City of Columbus Lawsuit Against Drug CompaniesDocument123 pagesCity of Columbus Lawsuit Against Drug CompaniesAnonymous AJEonl3yxjNo ratings yet
- Managing Pain: Key Considerations for NursesDocument7 pagesManaging Pain: Key Considerations for NursesMaria ArregoitiaNo ratings yet
- Edited: DR - Dairion Gatot M.Ked SP - PD-KHOMDocument57 pagesEdited: DR - Dairion Gatot M.Ked SP - PD-KHOMayuhati siregarNo ratings yet
- AnalgesicDocument3 pagesAnalgesicAnnaMaeVelosoNo ratings yet
- NC Opioid STR Final NarrativeDocument47 pagesNC Opioid STR Final NarrativeMistor WilliamsNo ratings yet
- Drug Study Morphine and ProtonixDocument3 pagesDrug Study Morphine and ProtonixHarvey Lampa SelimNo ratings yet
- Acute Management of Nephrolithiasis in Children - UpToDateDocument15 pagesAcute Management of Nephrolithiasis in Children - UpToDatedrtgodeNo ratings yet
- Pharmaceutical Chemistry Chapter 10 Analxtctycygestic and Anti Inflammatory Agents NotesDocument13 pagesPharmaceutical Chemistry Chapter 10 Analxtctycygestic and Anti Inflammatory Agents NotesBEST OF BESTNo ratings yet
- GM6052 – directed study: Pain materialsDocument52 pagesGM6052 – directed study: Pain materialsYohana VeronicaNo ratings yet
- Nursing Board Exam ReviewerDocument212 pagesNursing Board Exam Reviewerlevouge77793% (58)
- PercocetDocument1 pagePercocetAdrianne Bazo100% (1)
- Drug TraffickingDocument20 pagesDrug TraffickingUsman Ahmad TijjaniNo ratings yet
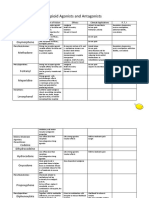
- Opioid Agonists and AntagonistsDocument5 pagesOpioid Agonists and AntagonistsCas BuNo ratings yet
- Pharmacology in Rehabilitation 4th EditionDocument682 pagesPharmacology in Rehabilitation 4th EditionSarah JaneNo ratings yet
- Pain Management DR ColeDocument8 pagesPain Management DR ColeAsep Cloud OvernightNo ratings yet
- Oet New Reading 1Document9 pagesOet New Reading 1Sanchit AbrolNo ratings yet
- Louis Harris - Problems of Drug Dependence 1991Document721 pagesLouis Harris - Problems of Drug Dependence 1991SmokeysamNo ratings yet
- CNS Drugs TextDocument27 pagesCNS Drugs TextTina TalmadgeNo ratings yet
- Drug StudyDocument3 pagesDrug StudyGail SantosNo ratings yet
- Codeine Phosphate TabDocument7 pagesCodeine Phosphate TabdeadscreamerzNo ratings yet
- 10 National Drug Iq ChallengeDocument4 pages10 National Drug Iq Challengeapi-309082881No ratings yet
- Drug StudyDocument23 pagesDrug StudyReiche GomezNo ratings yet