You might also like
- Transfusion of Blood & Blood Components1Document45 pagesTransfusion of Blood & Blood Components1Chamika Huruggamuwa100% (1)
- Blood TransfusionDocument28 pagesBlood TransfusionPORTRAIT OF A NURSENo ratings yet
- Blood and Blood ProductsDocument24 pagesBlood and Blood Productscnecardio100% (3)
- Blood Products: Product DescriptionDocument3 pagesBlood Products: Product Descriptionkaychi zNo ratings yet
- Pocket Guide On Red Cells 2012Document8 pagesPocket Guide On Red Cells 2012Dave OrlandoNo ratings yet
- Blood Groups & Blood BankingDocument36 pagesBlood Groups & Blood BankingGodfrey Pizaroh Mujuzi100% (2)
- Acquired Hemolytic Anemia Presentation For BPharmDocument24 pagesAcquired Hemolytic Anemia Presentation For BPharmHiren Pathak100% (2)
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocument44 pagesPractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarNo ratings yet
- University of Santo Tomas Immunohematology and Transfusion MedicineDocument7 pagesUniversity of Santo Tomas Immunohematology and Transfusion MedicineWynlor Abarca100% (1)
- Crossmatching and Issuing Blood Components PDFDocument20 pagesCrossmatching and Issuing Blood Components PDFdianaNo ratings yet
- Blood Transfusion and Transfusion ReactionDocument104 pagesBlood Transfusion and Transfusion Reactionrodelagapito-1100% (1)
- Blood Tranfusion11Document60 pagesBlood Tranfusion11Marites Angeles Bautista100% (2)
- Packed Cell Volume (PCV) TestDocument3 pagesPacked Cell Volume (PCV) TestchineduNo ratings yet
- Immunopharmacology: Dr. Hamad AlshabiDocument8 pagesImmunopharmacology: Dr. Hamad AlshabiHamad Alshabi100% (1)
- Compatibility Testing: Week 5Document33 pagesCompatibility Testing: Week 5Bridgette100% (1)
- Blood Administration: NRS 108 Essec County CollegeDocument22 pagesBlood Administration: NRS 108 Essec County CollegeDiah Puspita RiniNo ratings yet
- Heme Quiz 1-3Document14 pagesHeme Quiz 1-3Søren KierkegaardNo ratings yet
- Blood Donor Screening: Arce Lubang Bolima Mondoy Gocela Penero Bmls 4DDocument25 pagesBlood Donor Screening: Arce Lubang Bolima Mondoy Gocela Penero Bmls 4DMarj MendezNo ratings yet
- Typing, Screening and Crossmatching of BloodDocument55 pagesTyping, Screening and Crossmatching of BloodAsad MirzaNo ratings yet
- RH Blood Group SystemDocument18 pagesRH Blood Group SystemChristian John Mabalot Carillo50% (2)
- Collection of Blood From DonorsDocument7 pagesCollection of Blood From DonorsBernardoHernandezNo ratings yet
- Basics of ImmunohematologyDocument28 pagesBasics of ImmunohematologyAkhil ChaudharyNo ratings yet
- Blood Component TherapyDocument8 pagesBlood Component TherapyquerokeropiNo ratings yet
- Understanding CBC Histogram PDFDocument17 pagesUnderstanding CBC Histogram PDFSuresh ShresthaNo ratings yet
- WHO Blood Transfusion Safety GuidelinesDocument104 pagesWHO Blood Transfusion Safety GuidelinesrodelagapitoNo ratings yet
- RH Typing ReagentsDocument2 pagesRH Typing ReagentsMelanie Tomita100% (1)
- CryoprecipitateDocument7 pagesCryoprecipitateBrandon BNo ratings yet
- Blood Coagulation SeminarDocument115 pagesBlood Coagulation SeminarmeghaNo ratings yet
- Chapter 026 CoagulationDocument7 pagesChapter 026 Coagulationthubtendrolma100% (3)
- ORBCON-EN-BE Coagulation 02259Document24 pagesORBCON-EN-BE Coagulation 02259Леон Деспотоски100% (1)
- Human Platelet AntigenDocument56 pagesHuman Platelet AntigenMohandoss Murugesan100% (3)
- Intrauterine Fetal Transfusion of Red Blood CellsDocument16 pagesIntrauterine Fetal Transfusion of Red Blood CellsHervi LaksariNo ratings yet
- Lec 9-10 Blood Groups & TransfusionDocument51 pagesLec 9-10 Blood Groups & TransfusionEmily Peterson100% (1)
- Blood Transfusion Reactions: Dr. Madhuvan GuptaDocument42 pagesBlood Transfusion Reactions: Dr. Madhuvan GuptaDr. Madhuvan GuptaNo ratings yet
- Hemoglobin Electrophoresis1Document19 pagesHemoglobin Electrophoresis1nidaats100% (1)
- Hematology Lecture Notes PDFDocument102 pagesHematology Lecture Notes PDFMarisa IzzaNo ratings yet
- RBC AliquotsDocument1 pageRBC AliquotsARIF AHAMMEDNo ratings yet
- Hematology Multiple Choice Questions Guide StudentsDocument5 pagesHematology Multiple Choice Questions Guide StudentsMarie LlanesNo ratings yet
- Rapid Plasma Reagin (RPR) TestDocument5 pagesRapid Plasma Reagin (RPR) Testkiedd_04100% (3)
- Blood TransfusionDocument55 pagesBlood Transfusionanand7504100% (2)
- B Blab 6 Crossmatch SP 05Document14 pagesB Blab 6 Crossmatch SP 05Rutchelle Joyce PugoyNo ratings yet
- Transfusion ReactionsDocument28 pagesTransfusion ReactionsRovefrances ErpeluaNo ratings yet
- Interpret CBC Test Results and Diagnose Common Blood DisordersDocument39 pagesInterpret CBC Test Results and Diagnose Common Blood Disorderspido29No ratings yet
- Blood ComponentsDocument44 pagesBlood ComponentsKrisha VittoNo ratings yet
- Red Cell Antibody Panels InterpretationDocument40 pagesRed Cell Antibody Panels Interpretationrube10000No ratings yet
- Anti-Globulin Test ExplainedDocument5 pagesAnti-Globulin Test ExplainedfaeNo ratings yet
- A Complete Blood CountDocument6 pagesA Complete Blood CountecakimaNo ratings yet
- Antibody ScreeningDocument57 pagesAntibody ScreeningSebastian Jake John100% (1)
- HaemoglobinDocument47 pagesHaemoglobinPreethi AbhilashNo ratings yet
- Complete Blood Count: at A GlanceDocument6 pagesComplete Blood Count: at A Glancecsy123No ratings yet
- Quality Control in Clinical Biochemistry BMLTDocument56 pagesQuality Control in Clinical Biochemistry BMLTSelim JaforNo ratings yet
- Hematology 2 TEST QUESTIONSDocument4 pagesHematology 2 TEST QUESTIONSa a r o n b a u t i s t aNo ratings yet
- Acid base balance and electrolyte multiple choice questionsDocument56 pagesAcid base balance and electrolyte multiple choice questionsVirendra Joshi100% (1)
- Cross Matching-Wps OfficeDocument22 pagesCross Matching-Wps Officeashwini priyaNo ratings yet
- Red Blood Cell CountDocument5 pagesRed Blood Cell CountOmaNo ratings yet
- Blood Transfusion FinalDocument8 pagesBlood Transfusion FinalejkohNo ratings yet
- Blood Transfusion ENGLISHDocument40 pagesBlood Transfusion ENGLISHHajrahPalembangan100% (2)
- Total Leukocyte Count by HemocytometerDocument4 pagesTotal Leukocyte Count by HemocytometerMalkish RajkumarNo ratings yet
- ACL Technical Support Standard Script Append FilesDocument3 pagesACL Technical Support Standard Script Append FileswellawalalasithNo ratings yet
- ACL Technical Support Standard Script DocumentDocument4 pagesACL Technical Support Standard Script DocumentwellawalalasithNo ratings yet
- ACL Technical Support Standard Script Document: Page 1 of 3Document3 pagesACL Technical Support Standard Script Document: Page 1 of 3wellawalalasithNo ratings yet
- Audit Tests of Accounts Receivable Using ACL - Tests of Aged Trial BalanceDocument2 pagesAudit Tests of Accounts Receivable Using ACL - Tests of Aged Trial BalancewellawalalasithNo ratings yet
- Excel To Acl Cleanup Guide For Acl v.9Document9 pagesExcel To Acl Cleanup Guide For Acl v.9wellawalalasithNo ratings yet
- ACL Technical Support Standard Script Document: Page 1 of 3Document3 pagesACL Technical Support Standard Script Document: Page 1 of 3wellawalalasithNo ratings yet
- Append Many Files (Dir)Document3 pagesAppend Many Files (Dir)wellawalalasithNo ratings yet
- Acl Step by Step Instructions For Journal Entry TestingDocument52 pagesAcl Step by Step Instructions For Journal Entry TestingwellawalalasithNo ratings yet
- Excel Cleanup GuideDocument14 pagesExcel Cleanup GuidewellawalalasithNo ratings yet
- Excel To Acl Cleanup Guide For Acl v.9Document9 pagesExcel To Acl Cleanup Guide For Acl v.9wellawalalasithNo ratings yet
- Commonly Used ACL CommandsDocument6 pagesCommonly Used ACL CommandswellawalalasithNo ratings yet
- Acl Step by Step Instructions For Journal Entry TestingDocument52 pagesAcl Step by Step Instructions For Journal Entry TestingwellawalalasithNo ratings yet
- Worksheet - Income Sheet and Form Series 18 AICPA, AICPA Risk of Material Misstatement WorksheetsDocument20 pagesWorksheet - Income Sheet and Form Series 18 AICPA, AICPA Risk of Material Misstatement WorksheetswellawalalasithNo ratings yet
- Commonly Used ACL CommandsDocument6 pagesCommonly Used ACL CommandswellawalalasithNo ratings yet
- Excel Cleanup GuideDocument14 pagesExcel Cleanup GuidewellawalalasithNo ratings yet
- Statutory Provisions Part 03Document7 pagesStatutory Provisions Part 03wellawalalasithNo ratings yet
- Audit Tests of Accounts Receivable Using ACL - Tests of Aged Trial BalanceDocument2 pagesAudit Tests of Accounts Receivable Using ACL - Tests of Aged Trial BalancewellawalalasithNo ratings yet
- Making Materiality Judgment Practice StatementDocument48 pagesMaking Materiality Judgment Practice StatementwellawalalasithNo ratings yet
- Banking and Finance - Mortgage Servicing Rights, For The Specified Account. The Substantive Procedures Responsive To The RisksDocument19 pagesBanking and Finance - Mortgage Servicing Rights, For The Specified Account. The Substantive Procedures Responsive To The RiskswellawalalasithNo ratings yet
- Risk and Controls Guide - Banking and Finance - CashDocument20 pagesRisk and Controls Guide - Banking and Finance - CashwellawalalasithNo ratings yet
- Form 1840sdi-2 - Substantive Procedures Guide - Banking and Finance - LoansDocument17 pagesForm 1840sdi-2 - Substantive Procedures Guide - Banking and Finance - LoanswellawalalasithNo ratings yet
- TO: Chief Executive Officers of All Listed Companies Company Secretaries and Registrars of All Listed CompaniesDocument2 pagesTO: Chief Executive Officers of All Listed Companies Company Secretaries and Registrars of All Listed CompanieswellawalalasithNo ratings yet
- Form 18 Sdi 4 - Recourse Liabilities - Risk of Material Misstatement (Romm) WorksheetDocument17 pagesForm 18 Sdi 4 - Recourse Liabilities - Risk of Material Misstatement (Romm) WorksheetwellawalalasithNo ratings yet
- Risk of Material Misstatement Worksheet - Overview General InstructionsDocument26 pagesRisk of Material Misstatement Worksheet - Overview General InstructionswellawalalasithNo ratings yet
- Risk of Material Misstatement Worksheet - Overview General InstructionsDocument35 pagesRisk of Material Misstatement Worksheet - Overview General InstructionswellawalalasithNo ratings yet
- Statutory Provisions Part 04Document14 pagesStatutory Provisions Part 04wellawalalasithNo ratings yet
- Form 18 Sdi 2 - Loans - Risk of Material Misstatement (Romm) WorksheetDocument27 pagesForm 18 Sdi 2 - Loans - Risk of Material Misstatement (Romm) WorksheetwellawalalasithNo ratings yet
- SL3 – CORPORATE TAXATION STATUTORY PROVISIONSDocument12 pagesSL3 – CORPORATE TAXATION STATUTORY PROVISIONSwellawalalasithNo ratings yet
- Corporate Tax Recovery Provisions Under Sri Lankan LawDocument7 pagesCorporate Tax Recovery Provisions Under Sri Lankan LawwellawalalasithNo ratings yet
- Statutory Provisions Part 05Document12 pagesStatutory Provisions Part 05wellawalalasithNo ratings yet
- Ground Floor Supply Layout: Potable Hot & Cold General PlumbingDocument1 pageGround Floor Supply Layout: Potable Hot & Cold General PlumbingDanny ArimaNo ratings yet
- Physical Geology 2nd Edition Chapter 19 Climate ChangeDocument25 pagesPhysical Geology 2nd Edition Chapter 19 Climate ChangeMohammad Imran KhanNo ratings yet
- Badjao HouseDocument2 pagesBadjao HouseKim PapagNo ratings yet
- Chapter 7Document10 pagesChapter 7Christian U Rig-onNo ratings yet
- Bridge HydraulicsDocument222 pagesBridge HydraulicsAriffin NgahNo ratings yet
- Sharp Electrical Supply Offers Lighting EquipmentDocument2 pagesSharp Electrical Supply Offers Lighting Equipmentsherdan genistonNo ratings yet
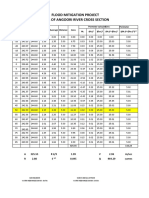
- Flood Mitigation Project Area of Angoori River Cross SectionDocument8 pagesFlood Mitigation Project Area of Angoori River Cross SectionankitNo ratings yet
- Aditya-L1 Mission: S. Seetha and S. MegalaDocument3 pagesAditya-L1 Mission: S. Seetha and S. MegalaJyoti YadavNo ratings yet
- Tropical and Sub-Tropical RegionDocument6 pagesTropical and Sub-Tropical RegionAnshul VermaNo ratings yet
- FP PNR, Pet, CT 1Document6 pagesFP PNR, Pet, CT 1adityaNo ratings yet
- Philippine Science 9 Periodical TestDocument5 pagesPhilippine Science 9 Periodical TestSarah Jane Nomo100% (1)
- Understanding Disaster Risk Reduction and ManagementDocument10 pagesUnderstanding Disaster Risk Reduction and ManagementSaralyn Mawallil AmilhamjaNo ratings yet
- Agridam ProgramDocument14 pagesAgridam ProgramBrian RascoNo ratings yet
- Diagrams & MapsDocument16 pagesDiagrams & MapsDrFouad AlgamalNo ratings yet
- What S The Weather LikeDocument2 pagesWhat S The Weather LikeStevens D Alexandro Gonzales AlarconNo ratings yet
- Weather WorksheetDocument1 pageWeather WorksheetIldikó Dimén0% (1)
- Joross Cleven Miguel Ruado: Tropical Cyclone Wind SignalsDocument2 pagesJoross Cleven Miguel Ruado: Tropical Cyclone Wind SignalsHelen SabuquelNo ratings yet
- Rainfed Agriculture and Watershed ManagementDocument18 pagesRainfed Agriculture and Watershed ManagementCH Rajan GujjarNo ratings yet
- 67-10th Social - Map Study Material - English Medium PDF DownloadDocument60 pages67-10th Social - Map Study Material - English Medium PDF DownloadannsNo ratings yet
- Converter Faults ProtectionDocument24 pagesConverter Faults ProtectionAmit BaliNo ratings yet
- DRRR Landslides and SinkholesDocument35 pagesDRRR Landslides and SinkholesGene Tecson50% (4)
- AWOS 3000 027 Maintenance Manual1 PDFDocument57 pagesAWOS 3000 027 Maintenance Manual1 PDFPham Van LinhNo ratings yet
- Volcano Model Guide QuestionsDocument1 pageVolcano Model Guide QuestionsMariel Niña Erasmo100% (2)
- Structural SteelDocument2 pagesStructural SteelZaher Mhd Sharaf100% (1)
- Aviation MCQsDocument5 pagesAviation MCQsMaqbool Khan67% (3)
- Mononobe Okabe EquationDocument3 pagesMononobe Okabe Equationnespak06No ratings yet
- Design Report J#685 Ircon Shell Store R1Document257 pagesDesign Report J#685 Ircon Shell Store R1chetanchintaNo ratings yet
- GallopingDocument5 pagesGallopingNagendra SinghNo ratings yet
- And Ocean Engineering, Vol. 116, No. 4, July /august, 1990. ©ASCE, ISSN 0733Document17 pagesAnd Ocean Engineering, Vol. 116, No. 4, July /august, 1990. ©ASCE, ISSN 0733Satheesh KumarNo ratings yet
- WFEFDocument17 pagesWFEFMahamadali DesaiNo ratings yet