You might also like
- How To Deal WithDocument65 pagesHow To Deal Withdr_asalehNo ratings yet
- Breast LumpDocument26 pagesBreast Lumpdr_asaleh100% (2)
- TrunkDocument86 pagesTrunkdr_asalehNo ratings yet
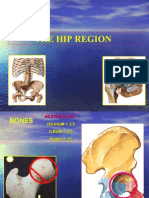
- Hip.www.1aim.netDocument60 pagesHip.www.1aim.netdr_asaleh100% (1)
- BoneDocument68 pagesBonedr_asaleh100% (2)
- Paediatric OrthopaedicDocument77 pagesPaediatric Orthopaedicdr_asalehNo ratings yet
- OrthopedicDocument71 pagesOrthopedicdr_asalehNo ratings yet
- Injuries Around TheDocument48 pagesInjuries Around Thedr_asalehNo ratings yet
- NeckDocument67 pagesNeckdr_asaleh100% (1)
- LongDocument64 pagesLongdr_asalehNo ratings yet
- Knee.www.1aim.netDocument34 pagesKnee.www.1aim.netdr_asalehNo ratings yet
- Examination of TheDocument29 pagesExamination of Thedr_asalehNo ratings yet
- Head and NeckDocument41 pagesHead and Neckdr_asalehNo ratings yet
- Upper ExtremityDocument33 pagesUpper Extremitydr_asalehNo ratings yet
- Elbow WristDocument59 pagesElbow Wristdr_asalehNo ratings yet
- Urinary IncontinenceDocument66 pagesUrinary Incontinencedr_asaleh100% (1)
- Bone JointDocument57 pagesBone Jointdr_asalehNo ratings yet
- Thoracic CavityDocument30 pagesThoracic Cavitydr_asalehNo ratings yet
- Anatomy Lecture1Document47 pagesAnatomy Lecture1dr_asalehNo ratings yet
- Skull, Brain, CNDocument60 pagesSkull, Brain, CNdr_asaleh100% (1)
- Head and NeckDocument41 pagesHead and Neckdr_asalehNo ratings yet
- The Lower Limb: Pelvis, Thigh, Leg and FootDocument27 pagesThe Lower Limb: Pelvis, Thigh, Leg and Footdr_asaleh100% (1)
- Contents of PelvisDocument38 pagesContents of Pelvisdr_asalehNo ratings yet
- AbdomenDocument11 pagesAbdomendr_asalehNo ratings yet
- Bones, Joints, MusclesDocument37 pagesBones, Joints, Musclesdr_asalehNo ratings yet
- Infertility IVDocument46 pagesInfertility IVdr_asalehNo ratings yet
- Artries and VeinsDocument25 pagesArtries and Veinsdr_asalehNo ratings yet
- Infertility IIIDocument72 pagesInfertility IIIdr_asalehNo ratings yet
- Menstrual Disorder and Abnormal BleedingDocument9 pagesMenstrual Disorder and Abnormal Bleedingdr_asalehNo ratings yet
- Infertility IIDocument58 pagesInfertility IIdr_asalehNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Patologi AnatomiDocument3 pagesPatologi Anatomidika anggrainniNo ratings yet
- Thyroid Case StudyDocument68 pagesThyroid Case Studyshadydogv5No ratings yet
- Endocrinology Question 1Document16 pagesEndocrinology Question 1BasirQidwai100% (4)
- Worksheet 1 - Endocrine - 2022 (11th Ed)Document4 pagesWorksheet 1 - Endocrine - 2022 (11th Ed)ahmadmahdi18mNo ratings yet
- Bald Thigh Syndrome of Greyhound Dogs - Gross and Microscopic FindingsDocument3 pagesBald Thigh Syndrome of Greyhound Dogs - Gross and Microscopic FindingsjenNo ratings yet
- An Introduction To Behavioral Endocrinol PDFDocument887 pagesAn Introduction To Behavioral Endocrinol PDFPaula100% (23)
- Sign of Hyperandrogenism PDFDocument6 pagesSign of Hyperandrogenism PDFmisbah_mdNo ratings yet
- What Is Adrenal InsufficiencyDocument17 pagesWhat Is Adrenal InsufficiencygammuacNo ratings yet
- Hypothyroidism Case AnalysisDocument3 pagesHypothyroidism Case AnalysisKrisianne Mae Lorenzo FranciscoNo ratings yet
- INS DT4 EN Ichroma™ T4 Rev.02Document4 pagesINS DT4 EN Ichroma™ T4 Rev.02Sami Al Samow0% (1)
- Plabable Gems Endocrine PDF P7aDocument44 pagesPlabable Gems Endocrine PDF P7aayşenur sevinçNo ratings yet
- ENDOCRINE DISORDERS (Autosaved)Document81 pagesENDOCRINE DISORDERS (Autosaved)Princewill SeiyefaNo ratings yet
- Exocrine Glands-Endocrine GlandsDocument8 pagesExocrine Glands-Endocrine GlandsneerleoNo ratings yet
- Progesterone and Estrogen Thyroid GlandDocument3 pagesProgesterone and Estrogen Thyroid GlandReymark VillanuevaNo ratings yet
- ThyrotoxicosisDocument16 pagesThyrotoxicosisFiorella Peña MoraNo ratings yet
- EndocrineDocument43 pagesEndocrineHirpâsà MămoNo ratings yet
- PosterDocument32 pagesPosterBeny RiliantoNo ratings yet
- Anfis Endokrin S2 (Compatibility Mode) .CompressedDocument66 pagesAnfis Endokrin S2 (Compatibility Mode) .CompressedAmiliya EmilNo ratings yet
- Menstrual Cycle Physiology: - Dr. Atef AboodDocument33 pagesMenstrual Cycle Physiology: - Dr. Atef AboodatefmaboodNo ratings yet
- Patients With Adrenal DisordersDocument17 pagesPatients With Adrenal DisordersTsarina Diana TanNo ratings yet
- Thyroid Disorders in Children and AdolescentsDocument12 pagesThyroid Disorders in Children and AdolescentsCharity TololiuNo ratings yet
- Synthesis and Functions of Steroid HormonesDocument54 pagesSynthesis and Functions of Steroid HormonesfanyazharNo ratings yet
- PCOSDocument4 pagesPCOSTp HoangNo ratings yet
- Mangement 2 PDFDocument165 pagesMangement 2 PDFjanveeNo ratings yet
- Preconception Counseling For Thyroid DisordersDocument7 pagesPreconception Counseling For Thyroid DisordersLiya AnjelinaNo ratings yet
- Essentials of Medical PhysiologyDocument6 pagesEssentials of Medical Physiologykumarraushan1000No ratings yet
- CH 5 Skin Practice TestDocument16 pagesCH 5 Skin Practice TestCrislyn MangubatNo ratings yet
- Clinical EndocrinologyDocument35 pagesClinical EndocrinologyBobskinny100% (1)
- Salivary Glands and Pancreas FunctionsDocument4 pagesSalivary Glands and Pancreas FunctionsAllen BurdowskiNo ratings yet
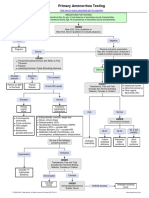
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet