You might also like
- Essential Guide to Skin Integrity and Wound CareDocument38 pagesEssential Guide to Skin Integrity and Wound CareMiu MiuNo ratings yet
- Wound Care PDFDocument100 pagesWound Care PDFVanessaMUeller100% (2)
- EnemaDocument2 pagesEnemaArjay AgravanteNo ratings yet
- Pharmacology of Gastrointestinal SystemDocument4 pagesPharmacology of Gastrointestinal SystemZaira KimNo ratings yet
- Maintaining Skin Integrity and Understanding Wound CareDocument146 pagesMaintaining Skin Integrity and Understanding Wound CareMichael Villavert100% (1)
- Dressing PDFDocument4 pagesDressing PDFIndika KarunamuniNo ratings yet
- What is an NCPDocument38 pagesWhat is an NCPSARAH DIANA ROSE S. MANALILI100% (1)
- Nursing Process (ADPIE) GuideDocument17 pagesNursing Process (ADPIE) GuidePRIYANo ratings yet
- Git HandoutsDocument49 pagesGit HandoutsCharlz Zipagan100% (1)
- Skin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxDocument92 pagesSkin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxAT4-11 HUMSS 2 CEDRICK ILAO100% (1)
- Physical Assessment of Skin, Hair and NailsDocument35 pagesPhysical Assessment of Skin, Hair and NailsRagna De HittaNo ratings yet
- Physical AssessmentDocument90 pagesPhysical AssessmentReann LeeNo ratings yet
- GI DisordersDocument62 pagesGI DisordersJeo Thomas100% (1)
- Hazards of IV TherapyDocument21 pagesHazards of IV TherapyFaraz Qurban RajperNo ratings yet
- Wound Dressing Guide PDFDocument2 pagesWound Dressing Guide PDFrufftuffcookieNo ratings yet
- Wound Care ChecklistDocument2 pagesWound Care ChecklistJay Lemuel BuenviajeNo ratings yet
- Heart & Neck Vessel AssessmentDocument46 pagesHeart & Neck Vessel AssessmentLouise Nathalia VelasquezNo ratings yet
- Introduction To The Musculoskeletal SystemDocument39 pagesIntroduction To The Musculoskeletal SystemdesyNo ratings yet
- Care of Patient With Respiratory DisordersDocument35 pagesCare of Patient With Respiratory Disorderskriiteeabns100% (1)
- MCN Skills Lab 2021Document25 pagesMCN Skills Lab 2021irene mancaoNo ratings yet
- Critical Care of Hyperglycemic Hyperosmolar Syndrome (HHNSDocument4 pagesCritical Care of Hyperglycemic Hyperosmolar Syndrome (HHNSJan Crizza Dale R. FrancoNo ratings yet
- Assessment of The Peripheral Vascular SystemDocument3 pagesAssessment of The Peripheral Vascular SystemTrisha Andrea DavaNo ratings yet
- A I. R R H: Bdomen Eview OF Elated IstoryDocument14 pagesA I. R R H: Bdomen Eview OF Elated Istorydlneisha61100% (1)
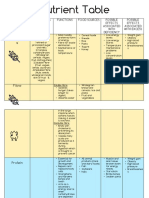
- Nutrient Table 2020Document8 pagesNutrient Table 2020Murphy MurphyNo ratings yet
- Oxygenation NotesDocument23 pagesOxygenation NoteschikaycNo ratings yet
- PsoriasisDocument27 pagesPsoriasisMala PotterNo ratings yet
- ChartingDocument1 pageChartingAdrianaMarreroNo ratings yet
- Learning Objective: - Explain of Acute AbdomenDocument143 pagesLearning Objective: - Explain of Acute AbdomenSamuel Sebastian SirapanjiNo ratings yet
- Care of The NewbornDocument41 pagesCare of The NewbornBaniwas Marie AgnesNo ratings yet
- NCM 118a Lec 9 Liver FailureDocument9 pagesNCM 118a Lec 9 Liver FailureJan Crizza Dale R. FrancoNo ratings yet
- Wound DressingDocument9 pagesWound Dressingapi-3722051100% (2)
- Heart Assessment GuideDocument54 pagesHeart Assessment GuideMa. Carissa Allaine SantosNo ratings yet
- Trauma and Emergency NursingDocument9 pagesTrauma and Emergency Nursingchinthaka18389021No ratings yet
- Nutrition SyllabusDocument4 pagesNutrition Syllabusapi-102106087No ratings yet
- Cell Ab Midterm MesiDocument7 pagesCell Ab Midterm MesiSamantha VeraNo ratings yet
- Irrigating A WoundDocument3 pagesIrrigating A Wounddate6No ratings yet
- Caring For The Woman Experiencing Complications During Labor and BirthDocument25 pagesCaring For The Woman Experiencing Complications During Labor and BirthJonalynCollodChewacheoNo ratings yet
- PharmacologyDocument9 pagesPharmacologyRPh Krishna Chandra JagritNo ratings yet
- Labor and Delivery Lecture NotesDocument14 pagesLabor and Delivery Lecture Notescolek22100% (22)
- Infectious Disease Awareness In, Mogadishu, SomaliaDocument7 pagesInfectious Disease Awareness In, Mogadishu, Somaliashafie Mohamed AliNo ratings yet
- Maternal ExamDocument52 pagesMaternal ExamRandyNo ratings yet
- Wound Care Management 1Document99 pagesWound Care Management 1Jan Oliver YaresNo ratings yet
- Perineal CareDocument3 pagesPerineal CareNikko Rafael RobillosNo ratings yet
- Stoma Management GuideDocument33 pagesStoma Management Guidepradeep nairNo ratings yet
- Intramuscular Injection GuidelinesDocument2 pagesIntramuscular Injection GuidelinesPauline MartinezNo ratings yet
- Demography and Globalization: WHY BE Concerned About Demography?Document7 pagesDemography and Globalization: WHY BE Concerned About Demography?Kristin Vera J. CaberteNo ratings yet
- M M M M: By: Jan Michael Khalid L. MacarambonDocument23 pagesM M M M: By: Jan Michael Khalid L. Macarambonxtaticboy82No ratings yet
- Care of WoundsDocument6 pagesCare of WoundsKimpoy Tu-osNo ratings yet
- Assessment of NewbornDocument26 pagesAssessment of Newbornaybee_14No ratings yet
- The Breasts & The AxillaeDocument26 pagesThe Breasts & The AxillaeMark Villarmea AlforqueNo ratings yet
- REVISED ADULT HEALTH ASSESSMENT FORM (2015) - GuideDocument13 pagesREVISED ADULT HEALTH ASSESSMENT FORM (2015) - GuideBianca MolinaNo ratings yet
- Assessing The Heart and Neck VesselsDocument6 pagesAssessing The Heart and Neck VesselsA R F I J U LNo ratings yet
- Assess Eyes, Ears, Nose, Mouth ExamDocument42 pagesAssess Eyes, Ears, Nose, Mouth ExamFranz Earl Niño AlbesaNo ratings yet
- Bed MakingDocument34 pagesBed Makingmunyamugracious100% (1)
- Hiatal HerniaDocument6 pagesHiatal HerniaElaine Jean UayanNo ratings yet
- Vital SignDocument40 pagesVital SignYoelBagusGiarto0% (1)
- Pressure Sore or Decubitus Ulcer or Bed SoreDocument20 pagesPressure Sore or Decubitus Ulcer or Bed SorePrecious BlessingNo ratings yet
- Tissue Integrity and Wound CarestudentDocument38 pagesTissue Integrity and Wound Carestudentbernard arcigaNo ratings yet
- Pressure UlcersDocument43 pagesPressure UlcersZubda Butt100% (2)
- Pressure Ulcers and Wounds: by Monica Warhaftig, D.O. Assistant Professor of Geriatrics N.S.UDocument64 pagesPressure Ulcers and Wounds: by Monica Warhaftig, D.O. Assistant Professor of Geriatrics N.S.UEvaNo ratings yet
- NCP BreastfeedingDocument3 pagesNCP Breastfeedingjam_robielos63% (8)
- Early Breastfeeding Experiences of AdoleDocument14 pagesEarly Breastfeeding Experiences of AdoleDivina D Galvez-BeronioNo ratings yet
- Selective Serotonin Reuptake Inhibitors - Past, Present and Future - S. Stanford (Landes, 1999) WWDocument237 pagesSelective Serotonin Reuptake Inhibitors - Past, Present and Future - S. Stanford (Landes, 1999) WWKitty CristinaNo ratings yet
- Nursing Practice Standards and CompetenciesDocument2 pagesNursing Practice Standards and CompetenciesDivina D Galvez-BeronioNo ratings yet
- The Experience of Breastfeeding in A Group of Teenage MothersDocument6 pagesThe Experience of Breastfeeding in A Group of Teenage MothersDivina D Galvez-BeronioNo ratings yet
- Nursing Act 1991 Intro PDFDocument2 pagesNursing Act 1991 Intro PDFPam Osido TumalaNo ratings yet
- Wound Care GuideDocument36 pagesWound Care GuideDivina D Galvez-BeronioNo ratings yet
- Promoting Protective Factors For Pregnant and Parenting Teens: A Guide For PractitionersDocument7 pagesPromoting Protective Factors For Pregnant and Parenting Teens: A Guide For PractitionersDivina D Galvez-BeronioNo ratings yet
- Breast Versus BottleDocument8 pagesBreast Versus BottleDivina D Galvez-BeronioNo ratings yet
- Health Teaching About BreastfeedingDocument2 pagesHealth Teaching About BreastfeedingDivina D Galvez-BeronioNo ratings yet
- Breastfeeding Behavior Amog AdolescentDocument17 pagesBreastfeeding Behavior Amog AdolescentDivina D Galvez-BeronioNo ratings yet
- Reviewer NIODocument17 pagesReviewer NIODivina D Galvez-BeronioNo ratings yet
- RN Vs RPN PDFDocument20 pagesRN Vs RPN PDFDivina D Galvez-BeronioNo ratings yet
- Professional StandardsDocument16 pagesProfessional StandardsDivina D Galvez-BeronioNo ratings yet
- The Experience of Breastfeeding in A Group of Teenage MothersDocument6 pagesThe Experience of Breastfeeding in A Group of Teenage MothersDivina D Galvez-BeronioNo ratings yet
- Infant Feeding Practices of Young MothersDocument6 pagesInfant Feeding Practices of Young MothersDivina D Galvez-BeronioNo ratings yet
- BSRC Breastfeeding Factsheet 3 ENGDocument5 pagesBSRC Breastfeeding Factsheet 3 ENGDivina D Galvez-BeronioNo ratings yet
- Health Assessment GenitalDocument11 pagesHealth Assessment GenitalDivina D Galvez-BeronioNo ratings yet
- Mothers'Breastfeedng ExperiencesDocument11 pagesMothers'Breastfeedng ExperiencesDivina D Galvez-BeronioNo ratings yet
- Carolina Maria de Sá Guimarães, Raquel Germano Conde, Bruna Cremasco de Brito, Flávia Azevedo Gomes-Sponholz, Mônica Oliveira Batista Oriá, Juliana Cristina Dos Santos MonteiroDocument9 pagesCarolina Maria de Sá Guimarães, Raquel Germano Conde, Bruna Cremasco de Brito, Flávia Azevedo Gomes-Sponholz, Mônica Oliveira Batista Oriá, Juliana Cristina Dos Santos MonteiroDivina D Galvez-BeronioNo ratings yet
- OutDocument9 pagesOutDivina D Galvez-BeronioNo ratings yet
- Icas PhilDocument2 pagesIcas PhilDivina D Galvez-BeronioNo ratings yet
- The Therapeutic Nurse-Client RelationshipDocument10 pagesThe Therapeutic Nurse-Client RelationshipDivina D Galvez-BeronioNo ratings yet
- But Is It A Normal Thing?' Teenage Mothers' Experiences of Breastfeeding Promotion and SupportDocument7 pagesBut Is It A Normal Thing?' Teenage Mothers' Experiences of Breastfeeding Promotion and SupportDivina D Galvez-BeronioNo ratings yet
- Privacy and Confidentiality OverviewDocument17 pagesPrivacy and Confidentiality OverviewDivina D Galvez-BeronioNo ratings yet
- Directives: PR Actice GuidelineDocument8 pagesDirectives: PR Actice GuidelineDivina D Galvez-BeronioNo ratings yet
- Erik EriksonDocument6 pagesErik EriksonDivina D Galvez-BeronioNo ratings yet
- Accountability PDFDocument24 pagesAccountability PDFDivina GalvezNo ratings yet
- Professional StandardsDocument16 pagesProfessional StandardsDivina D Galvez-BeronioNo ratings yet
- RN Vs RPN PDFDocument20 pagesRN Vs RPN PDFDivina D Galvez-BeronioNo ratings yet
- NCP Skin IntegityDocument3 pagesNCP Skin Integityclydell joyce masiarNo ratings yet
- Herbal Plants: Keeping Our Traditional Wisdom AliveDocument16 pagesHerbal Plants: Keeping Our Traditional Wisdom AliveDeaths ComingNo ratings yet
- Initial Assessment and Management of TraumaDocument40 pagesInitial Assessment and Management of Traumayunita murfhiNo ratings yet
- 10 Herbal Meds in PhilippinesDocument12 pages10 Herbal Meds in PhilippinesRei Anne Adducul Ancheta100% (1)
- Second Degree Burns: The Key Ingredients:: Marketability Product DescriptionDocument1 pageSecond Degree Burns: The Key Ingredients:: Marketability Product DescriptionBenhazen Lynn DeirdreNo ratings yet
- Diabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSDocument20 pagesDiabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSPrashant LokhandeNo ratings yet
- Guava Leaves Extract As Main Ingredient in Making Herbal Soap For Washing WoundsDocument5 pagesGuava Leaves Extract As Main Ingredient in Making Herbal Soap For Washing WoundsKurt ReyesNo ratings yet
- Operating Instructions: Inspection Machine CUB Machine Number: I 1347Document116 pagesOperating Instructions: Inspection Machine CUB Machine Number: I 1347Justine MarashanyeNo ratings yet
- Stop The Bleed BookletDocument16 pagesStop The Bleed Bookletepraetorian100% (1)
- GUARDS - BASIC - COURSE - PACKAGE (1) EDIT With CSMDocument134 pagesGUARDS - BASIC - COURSE - PACKAGE (1) EDIT With CSMEmmanuel A. MirimboNo ratings yet
- Healing of Hymenal Injuries in Prepubertal and Adolescent Girls: A Descriptive StudyDocument15 pagesHealing of Hymenal Injuries in Prepubertal and Adolescent Girls: A Descriptive Studyhendrik septianaNo ratings yet
- Criminalistics Reviewer 3Document3 pagesCriminalistics Reviewer 3fmroyalNo ratings yet
- Teaching Plan Wound CareDocument3 pagesTeaching Plan Wound CareLody Lean CruzNo ratings yet
- Infection & Specific Wound InfectionsDocument39 pagesInfection & Specific Wound InfectionsAhmed ShorshNo ratings yet
- Rehabilitation For Persons With Upper Extremity AmputationDocument14 pagesRehabilitation For Persons With Upper Extremity AmputationVince ObiedoNo ratings yet
- Application of Panchakarma in Shalya Tantra A ReviewDocument5 pagesApplication of Panchakarma in Shalya Tantra A ReviewEditor IJTSRDNo ratings yet
- Blunt Force Trauma: Slide 1Document19 pagesBlunt Force Trauma: Slide 1Achmad MuflihNo ratings yet
- Sterile Suture Techniques Instruction SetDocument6 pagesSterile Suture Techniques Instruction Setcyc5326No ratings yet
- WOUNDS National Stakeholder Round-Table ReportDocument17 pagesWOUNDS National Stakeholder Round-Table Reportmaureen_latockiNo ratings yet
- Health 9 Learning Activity Sheet Quarter 3, Week 2-5 Content Standard: Performance Standard: Learning CompetencyDocument7 pagesHealth 9 Learning Activity Sheet Quarter 3, Week 2-5 Content Standard: Performance Standard: Learning Competencyfe delgadoNo ratings yet
- Open Injury ClassificationDocument6 pagesOpen Injury ClassificationSivaprasath JaganathanNo ratings yet
- Post Operative Emergency Management in Periodontics PeioDocument40 pagesPost Operative Emergency Management in Periodontics PeioFourthMolar.comNo ratings yet
- Wound Healing and Guava LeavesDocument5 pagesWound Healing and Guava LeavesTish Shamir MonisNo ratings yet
- The GP Book KeralaDocument108 pagesThe GP Book KeralaTejas Shah91% (47)
- Achilles Tendon Ruptures from Kite String InjuriesDocument4 pagesAchilles Tendon Ruptures from Kite String InjuriessyahmiNo ratings yet
- Wound 2016 0720Document10 pagesWound 2016 0720Lucky Permana100% (1)
- The Healing Effect of Amniotic Membrane in Burn PatientsDocument6 pagesThe Healing Effect of Amniotic Membrane in Burn PatientsInggrid Ayusari AsaliNo ratings yet
- The GP Note 2020Document306 pagesThe GP Note 2020firdauseahNo ratings yet
- Management of Clients With Burns and ShockDocument7 pagesManagement of Clients With Burns and ShockJunah Marie Rubinos Palarca0% (1)
- Subcutaneous InjectionDocument5 pagesSubcutaneous InjectionNovita sariNo ratings yet