You might also like
- ARDSDocument28 pagesARDSKAMLESH RATHODNo ratings yet
- Acute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarDocument47 pagesAcute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarAsri PrameswariNo ratings yet
- Prezentare Caz Clinic Ventilatia Mecanica IntraoperatorieDocument55 pagesPrezentare Caz Clinic Ventilatia Mecanica Intraoperatorieralucaioana89No ratings yet
- 2021-11 Jenny's PARDS PresentationDocument33 pages2021-11 Jenny's PARDS PresentationJenny WoodruffNo ratings yet
- AssccDocument96 pagesAssccFirdaus AzinunNo ratings yet
- Ards PDFDocument73 pagesArds PDFdr.Nugroho PrasetyoNo ratings yet
- Mechanical VentilationDocument19 pagesMechanical VentilationAashay DwivediNo ratings yet
- Treatment of ARDS: Ventilation, Fluids, NutritionDocument15 pagesTreatment of ARDS: Ventilation, Fluids, Nutritionf3wlNo ratings yet
- ArdsDocument26 pagesArdsMarkendey KhannaNo ratings yet
- Ards (Acute Respiratory Distress Syndrome)Document25 pagesArds (Acute Respiratory Distress Syndrome)sisNo ratings yet
- Critical Care Anesthesiology: A Concise OverviewDocument54 pagesCritical Care Anesthesiology: A Concise Overviewamir pouyaNo ratings yet
- Critical Care Anesthesiology: Dr. Navid Shafigh Fellowship of Critical Care MedicineDocument54 pagesCritical Care Anesthesiology: Dr. Navid Shafigh Fellowship of Critical Care Medicineamir pouyaNo ratings yet
- Dr Mohammed Jamsheed's Guide to Acute Respiratory Distress Syndrome (ARDSDocument53 pagesDr Mohammed Jamsheed's Guide to Acute Respiratory Distress Syndrome (ARDSavicennax100% (1)
- Acute Respiratory Distress SyndromeDocument18 pagesAcute Respiratory Distress SyndromeIrham TahkikNo ratings yet
- Acute Pulmonary FailureDocument15 pagesAcute Pulmonary FailureMariahnaSadjaluddinNo ratings yet
- Hypoxemic Respiratory FailureDocument70 pagesHypoxemic Respiratory FailureMohamed Rikarz Ahamed RikarzNo ratings yet
- ARDS - 1 - FinalDocument45 pagesARDS - 1 - FinalRoseNo ratings yet
- ARDS Respiratory Distress Syndrome Diagnosis Treatment PrognosisDocument24 pagesARDS Respiratory Distress Syndrome Diagnosis Treatment PrognosisPooja ShashidharanNo ratings yet
- Acute Respiratory Distress SyndromeDocument26 pagesAcute Respiratory Distress Syndromethea waaniNo ratings yet
- ARDS PresentationDocument89 pagesARDS Presentationalexandriaputera30No ratings yet
- Acute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNDocument59 pagesAcute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNAboodsha ShNo ratings yet
- 2016-1014 ARDS Update v3.0Document75 pages2016-1014 ARDS Update v3.0Edwin CvNo ratings yet
- Mechnical Vent New - PPT 1Document61 pagesMechnical Vent New - PPT 1الغائب الحاضرNo ratings yet
- 1 s2.0 S0735675721010184 MainDocument3 pages1 s2.0 S0735675721010184 Mainerandi hernandezNo ratings yet
- ARDS / COVID General ManagementDocument45 pagesARDS / COVID General ManagementJoe WildNo ratings yet
- ARDSDocument29 pagesARDSSwee ShiuanNo ratings yet
- Aha Ventilación Módulo 4Document10 pagesAha Ventilación Módulo 4Juan Carlos GomezNo ratings yet
- Yoshiaki Uda ICU Presentation 14/4/2010Document19 pagesYoshiaki Uda ICU Presentation 14/4/2010yoshiudaNo ratings yet
- Intra-Operative PEEP Vs ZEEPDocument37 pagesIntra-Operative PEEP Vs ZEEPMohamed RifanNo ratings yet
- BTS 2017 OXY LIỆU PHÁP- Slide Set for DoctorsDocument64 pagesBTS 2017 OXY LIỆU PHÁP- Slide Set for DoctorsNguyen ThinhNo ratings yet
- Hyperbaric Oxygen Therapy: DR Deepak Kumar Lady Hardinge Medical CollegeDocument52 pagesHyperbaric Oxygen Therapy: DR Deepak Kumar Lady Hardinge Medical CollegeAshitha S KabeerNo ratings yet
- Copd (Chronic Obstructive: Pulmonary Disease)Document68 pagesCopd (Chronic Obstructive: Pulmonary Disease)sinan kNo ratings yet
- Acute Respiratory Distress SyndromeDocument31 pagesAcute Respiratory Distress Syndromegretchen marie100% (1)
- Lung Expansion TherapyDocument108 pagesLung Expansion TherapyJean NoronhaNo ratings yet
- Respiratory Failure PresentationDocument13 pagesRespiratory Failure PresentationHusnain Irshad AlviNo ratings yet
- ERS Short Guidelines On COVID 19 ManagementDocument56 pagesERS Short Guidelines On COVID 19 ManagementDicky WahyudiNo ratings yet
- ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) DEFINITION AND MANAGEMENTDocument30 pagesACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) DEFINITION AND MANAGEMENTamalia adeNo ratings yet
- Acute Respiratory Distress SyndromeDocument18 pagesAcute Respiratory Distress SyndromeNitnotGundilNo ratings yet
- Oxygen Therapy DR RSWDocument61 pagesOxygen Therapy DR RSWdr.chotimatulhusnaNo ratings yet
- 2 O2 Therapy 2021Document58 pages2 O2 Therapy 2021Marceline GarciaNo ratings yet
- Asit Baz 2Document50 pagesAsit Baz 2Sarper Hikmet TAZENo ratings yet
- Hypoxemia in ICU: Prepared by Hadi JazanDocument41 pagesHypoxemia in ICU: Prepared by Hadi JazanHadi JazanNo ratings yet
- Management of ARDSDocument57 pagesManagement of ARDSRajaNo ratings yet
- Respiratory Failure: by ArDocument39 pagesRespiratory Failure: by ArAleksei RomahovNo ratings yet
- Oxygen TherapyDocument20 pagesOxygen TherapyBeri NyuydzefonNo ratings yet
- Prone Position Guidelines-2Document14 pagesProne Position Guidelines-2SAMINo ratings yet
- Respiratory Failure: Sa'ad Lahri Registrar Dept of Emergency Medicine UCT / University of StellenboschDocument18 pagesRespiratory Failure: Sa'ad Lahri Registrar Dept of Emergency Medicine UCT / University of StellenboschpolushkyNo ratings yet
- Airway ManagementDocument30 pagesAirway ManagementFuad TalNo ratings yet
- NSG261Oxygen GasexchangeDocument39 pagesNSG261Oxygen Gasexchangekatherine chippsNo ratings yet
- Oxygen Therapy: Skills and ProceduresDocument87 pagesOxygen Therapy: Skills and ProceduresVIA GABRIELLE OCENARNo ratings yet
- Cpap - IanDocument20 pagesCpap - IananggrainiNo ratings yet
- CH 19-Noninvasive VentilationDocument65 pagesCH 19-Noninvasive VentilationGhaida AlshehriNo ratings yet
- Adult Respiratory Distress Syndrome-StpDocument34 pagesAdult Respiratory Distress Syndrome-StpericNo ratings yet
- Mechanical VentilationDocument13 pagesMechanical VentilationNithiya NadesanNo ratings yet
- Adult Respiratory Distress Syndrome ManagementDocument51 pagesAdult Respiratory Distress Syndrome ManagementArsitoNo ratings yet
- Acute respiratory distress syndromeDocument2 pagesAcute respiratory distress syndromeSNo ratings yet
- Mechanical Ventilation Handout - AllenhoDocument23 pagesMechanical Ventilation Handout - AllenhoTahani SulNo ratings yet
- COPD Treatment and Dental CareDocument42 pagesCOPD Treatment and Dental CareAnoos rabayarabayaNo ratings yet
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- Finding and Reviewing Research Evidence in The: LiteratureDocument34 pagesFinding and Reviewing Research Evidence in The: LiteratureAmani KayedNo ratings yet
- L3Document35 pagesL3Amani KayedNo ratings yet
- L5 PDFDocument64 pagesL5 PDFAmani KayedNo ratings yet
- L6Document32 pagesL6Amani KayedNo ratings yet
- L5 PDFDocument64 pagesL5 PDFAmani KayedNo ratings yet
- L1Document49 pagesL1Amani KayedNo ratings yet
- L2Document27 pagesL2Amani KayedNo ratings yet
- L8Document40 pagesL8Amani Kayed0% (1)
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani KayedNo ratings yet
- L10Document92 pagesL10Amani KayedNo ratings yet
- L7Document53 pagesL7Amani KayedNo ratings yet
- ECG Dysrhythmias IIDocument23 pagesECG Dysrhythmias IIAmani KayedNo ratings yet
- Intrapartum Nursing Assessment + The Family in Childbirth: Needs and CareDocument59 pagesIntrapartum Nursing Assessment + The Family in Childbirth: Needs and CareAmani KayedNo ratings yet
- L9Document60 pagesL9Amani KayedNo ratings yet
- The Family in Childbirth: Needs and Care: Fourth EditionDocument21 pagesThe Family in Childbirth: Needs and Care: Fourth EditionAmani KayedNo ratings yet
- Chapter 15 - EN and PNDocument38 pagesChapter 15 - EN and PNAmani KayedNo ratings yet
- Basic Cardiac Dysrhythmias GuideDocument25 pagesBasic Cardiac Dysrhythmias GuideAmani KayedNo ratings yet
- Chapter 15 - EN and PNDocument38 pagesChapter 15 - EN and PNAmani KayedNo ratings yet
- Chapter 4lipids PDFDocument75 pagesChapter 4lipids PDFAmani KayedNo ratings yet
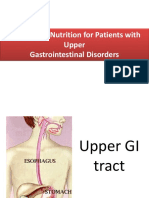
- Nutrition Therapy for Upper GI DisordersDocument34 pagesNutrition Therapy for Upper GI DisordersAmani KayedNo ratings yet
- Chapter 18 - Lower GIDocument71 pagesChapter 18 - Lower GIAmani KayedNo ratings yet
- Chapter 3: Proteins: in Greek: "To Take First Place"Document52 pagesChapter 3: Proteins: in Greek: "To Take First Place"Amani KayedNo ratings yet
- Chapter 1 - Nursing and Nutrition PDFDocument47 pagesChapter 1 - Nursing and Nutrition PDFAmani KayedNo ratings yet
- Chapter 5 & 6Document67 pagesChapter 5 & 6Amani KayedNo ratings yet
- Dental FluorosisDocument8 pagesDental Fluorosiskuantumonline100% (1)
- Tooth Size Discrepancies in An Orthodontic PopulationDocument7 pagesTooth Size Discrepancies in An Orthodontic PopulationUniversity Malaya's Dental Sciences ResearchNo ratings yet
- Claude H. Organ, JRDocument3 pagesClaude H. Organ, JRgassun2999No ratings yet
- Skull Base Course BrochureDocument3 pagesSkull Base Course BrochureEslam KandilNo ratings yet
- Camp Rap-A-Hope - 2013 Annual ReportDocument20 pagesCamp Rap-A-Hope - 2013 Annual ReportWest SandersNo ratings yet
- Cleft Lip and Palate CareDocument16 pagesCleft Lip and Palate CareIsmail LubisNo ratings yet
- Usaf Nurse Corps-Information Booklet-4feb13Document39 pagesUsaf Nurse Corps-Information Booklet-4feb13Jorge Vigoreaux100% (1)
- Arch Length Changes from Infancy to Mid-AdulthoodDocument6 pagesArch Length Changes from Infancy to Mid-AdulthoodLiceth Herrera MartinezNo ratings yet
- Infant Formula and Early Childhood CariesDocument5 pagesInfant Formula and Early Childhood Cariesmutiara hapkaNo ratings yet
- A Review of Root Fractures Diagnosis Treatment andDocument10 pagesA Review of Root Fractures Diagnosis Treatment andAya Ibrahim YassinNo ratings yet
- Queensland RMO Application GuideDocument18 pagesQueensland RMO Application GuideSOMANATHAN UMAHSUTHANNo ratings yet
- ChronOS InjecDocument24 pagesChronOS Injecmolecule112No ratings yet
- Trigger Point Techniques - What Is NAT - Niel Asher HealthcareDocument17 pagesTrigger Point Techniques - What Is NAT - Niel Asher Healthcaresalmazz0% (1)
- 3 - ALR Main - DoigtsDocument62 pages3 - ALR Main - DoigtsProfesseur Christian Dumontier100% (1)
- History Taking and Clinical ExaminationDocument34 pagesHistory Taking and Clinical Examinationrinaldi100% (1)
- FC Path (SA) Anat Part II Past Papers - 2011 Sept 7-7-2014Document4 pagesFC Path (SA) Anat Part II Past Papers - 2011 Sept 7-7-2014matentenNo ratings yet
- AyurvedaDocument1 pageAyurvedayuvi087No ratings yet
- Slide Tentang Bite Plane PDFDocument3 pagesSlide Tentang Bite Plane PDFRahmat HidayatNo ratings yet
- Recent Developments in The Management of Neonatal HyperbilirubinemiaDocument8 pagesRecent Developments in The Management of Neonatal HyperbilirubinemiaMyrtle SetiawanNo ratings yet
- Management of Early Onset FGR - A. BaschatDocument4 pagesManagement of Early Onset FGR - A. BaschatLokesh KhuranaNo ratings yet
- Short Answer Questions in Anaesthesia 2nd EdnDocument1 pageShort Answer Questions in Anaesthesia 2nd Edniahmad9No ratings yet
- 15 - 52 - 456 - Design & Development of A System For Nadi ParikshaDocument6 pages15 - 52 - 456 - Design & Development of A System For Nadi ParikshajananiNo ratings yet
- Injuries in YogaDocument30 pagesInjuries in YogaKalpak Shah100% (1)
- Daftar Pustaka KBDocument3 pagesDaftar Pustaka KBYogi OktiandiNo ratings yet
- Anatomy of Anterior Chamber Angle and Physiology ofDocument24 pagesAnatomy of Anterior Chamber Angle and Physiology ofAnumeha Jindal100% (1)
- Fortis HealthcareDocument20 pagesFortis Healthcareश्रीराम Venkat100% (1)
- 99 Day Study Schedule For USMLE Step 1 PDFDocument27 pages99 Day Study Schedule For USMLE Step 1 PDFAhmad JaleelNo ratings yet
- Josephine Ball ResumeDocument1 pageJosephine Ball Resumeapi-483700218No ratings yet
- Evaluación Manual Del DiafragmaDocument8 pagesEvaluación Manual Del DiafragmaSilvia Victoria SavaroNo ratings yet
- Hands On Ivf Training - Chennai Fertility Centre - Chennai, India, DR - VM.ThomasDocument21 pagesHands On Ivf Training - Chennai Fertility Centre - Chennai, India, DR - VM.ThomasThomasVadingaduNo ratings yet