You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- High CholesterolDocument31 pagesHigh Cholesterolashoku2100% (1)
- Clinical Chemistry Reviewer by MTRDocument56 pagesClinical Chemistry Reviewer by MTRRyan Pan95% (19)
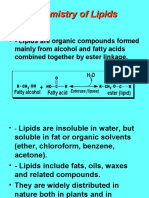
- Chemistry of LipidsDocument88 pagesChemistry of LipidsDanielle Anne Zamora-Matillosa LambanNo ratings yet
- TES Harian: Bahasa InggrisDocument3 pagesTES Harian: Bahasa InggrisZaid Al KhoirNo ratings yet
- Preparation of Soyabean Milk and Its Comparison With Natural MilkDocument18 pagesPreparation of Soyabean Milk and Its Comparison With Natural MilkVani AdigaNo ratings yet
- Chemistry Paper 3 Tz1 HL MarkschemeDocument22 pagesChemistry Paper 3 Tz1 HL MarkschemeIwona Agata GórnickaNo ratings yet
- Giles Set CDocument45 pagesGiles Set CPrinting CoNo ratings yet
- Research Grade 10 JDDocument45 pagesResearch Grade 10 JDDanielle DanielleNo ratings yet
- Healthmedicinet I 2016 10Document397 pagesHealthmedicinet I 2016 10tuni santeNo ratings yet
- Lab Values, Normal Adult - Laboratory Reference Ranges in Healthy AdultsDocument7 pagesLab Values, Normal Adult - Laboratory Reference Ranges in Healthy Adultsozoemena29No ratings yet
- Artikel 1Document11 pagesArtikel 1wardatul UllyaNo ratings yet
- Insert Kit LDLDocument6 pagesInsert Kit LDLsarah alatasNo ratings yet
- Saturated Fats and Health: A Reassessment and Proposal For Food-Based RecommendationsDocument14 pagesSaturated Fats and Health: A Reassessment and Proposal For Food-Based RecommendationsMónika BokorNo ratings yet
- 02 Synergy Book (English) PDFDocument34 pages02 Synergy Book (English) PDFAkmal RushdiNo ratings yet
- Singkatan Arti Atau Kepanjangan DI LABORATORIUMDocument6 pagesSingkatan Arti Atau Kepanjangan DI LABORATORIUMDIANNo ratings yet
- Use Your Brain To Change Your Age by Daniel G. Amen - ExcerptDocument38 pagesUse Your Brain To Change Your Age by Daniel G. Amen - ExcerptCrown Publishing Group89% (9)
- Research Paper 2017 2019 FDocument53 pagesResearch Paper 2017 2019 FKim Iryz Idmilao50% (2)
- Managing CholesterolDocument16 pagesManaging CholesterolGiannis Karp100% (2)
- Tugas ApolipoproteinDocument8 pagesTugas ApolipoproteinSeptiany Christin PalilinganNo ratings yet
- 2016 Adipose Tissue Hyperplasia With Enhanced Adipocyte-Derived Stem Cell Activity in Tc1 (C8orf4) - Deleted MiceDocument10 pages2016 Adipose Tissue Hyperplasia With Enhanced Adipocyte-Derived Stem Cell Activity in Tc1 (C8orf4) - Deleted MiceFrancisco Antonó Castro WeithNo ratings yet
- Bempedoic Acid: 06-Feb-2020 CreatedDocument56 pagesBempedoic Acid: 06-Feb-2020 CreatedLuis Carlos MillánNo ratings yet
- Antihyperlipidemic AgentsDocument71 pagesAntihyperlipidemic AgentsFirda100% (1)
- Cardiovascular Disease PHD ThesisDocument6 pagesCardiovascular Disease PHD Thesisafknawjof100% (2)
- Metabolic Syndrome and StrokeDocument5 pagesMetabolic Syndrome and StrokeEmir SaricNo ratings yet
- SIPDocument35 pagesSIPDemi RaeNo ratings yet
- 90 Day Journal DigitalDocument283 pages90 Day Journal DigitalDulcineaa90% (10)
- Formal Report Extraction of Total Lipids From Chicken Egg Yolk and ColumnDocument4 pagesFormal Report Extraction of Total Lipids From Chicken Egg Yolk and ColumnNorjem Villanueva88% (8)
- Neutriderm Moisturising LotionDocument13 pagesNeutriderm Moisturising LotionUASPharmaceuticalsNo ratings yet
- Fat PTC8Document52 pagesFat PTC8vNo ratings yet
- The PILOT - January 2022Document24 pagesThe PILOT - January 2022RSCA Redwood ShoresNo ratings yet