You might also like
- Cardiopulmonary Exercise Testing - Harshith - Apr 2018Document75 pagesCardiopulmonary Exercise Testing - Harshith - Apr 2018GeoNo ratings yet
- Cardio Notes, Heart FailureDocument17 pagesCardio Notes, Heart FailureJoy DunwanNo ratings yet
- Cardiovascular System: Presented byDocument76 pagesCardiovascular System: Presented bySoma Al-mutairiNo ratings yet
- Heart Failure and ShockDocument34 pagesHeart Failure and Shockfrenee aradanasNo ratings yet
- Nursing Study GuideDocument21 pagesNursing Study GuideYanahNo ratings yet
- Congestive Heart FailureDocument14 pagesCongestive Heart Failurelolo0880No ratings yet
- Assessment & Reasoning Cardiac System: Suggested Cardiac Nursing Assessment Skills To Be DemonstratedDocument8 pagesAssessment & Reasoning Cardiac System: Suggested Cardiac Nursing Assessment Skills To Be DemonstratedSharon Tanveer100% (1)
- Exercise TestingDocument50 pagesExercise TestingGeoNo ratings yet
- Essential Guide to Heart FailureDocument59 pagesEssential Guide to Heart FailureMahesh RathnayakeNo ratings yet
- (Pathophysiology, Types & MGT) : ShockDocument37 pages(Pathophysiology, Types & MGT) : ShockApriliani Nur Puspita SariNo ratings yet
- Heart Failure: Definition, Etiology and PathophysiologyDocument108 pagesHeart Failure: Definition, Etiology and PathophysiologySianipar RomulussNo ratings yet
- Med-Surge Study GuideDocument39 pagesMed-Surge Study Guidefbernis1480_11022046No ratings yet
- DYSPNEADocument37 pagesDYSPNEAdr. snehal patilNo ratings yet
- Congestive Heart FailureDocument39 pagesCongestive Heart FailureEthiopia TekdemNo ratings yet
- Cpet by Karlman Wasserman 2019Document76 pagesCpet by Karlman Wasserman 2019Wafa Naseem SheikhNo ratings yet
- MEDICAL PATHOLOGIES - CardiovascularDocument6 pagesMEDICAL PATHOLOGIES - Cardiovascularngachangong victorineNo ratings yet
- Shock Types 141009102815 Conversion Gate01Document41 pagesShock Types 141009102815 Conversion Gate01Samjaisheel SamsonNo ratings yet
- Introduction To ShockDocument56 pagesIntroduction To ShockPaolo VegaNo ratings yet
- Congestive Heart FailureDocument25 pagesCongestive Heart Failuredexter veracityNo ratings yet
- Understanding Cardiovascular DisordersDocument133 pagesUnderstanding Cardiovascular DisordersYashvi SinghNo ratings yet
- HF DeaDocument53 pagesHF DeaSyifa Mahmud Syukran AkbarNo ratings yet
- Lec 3 Heart FailureDocument25 pagesLec 3 Heart FailureDelete AccountNo ratings yet
- Cardiogenic Shock ManagementDocument66 pagesCardiogenic Shock ManagementdrkurniatiNo ratings yet
- Mitral RegurgitationDocument43 pagesMitral Regurgitationraissasafitry100% (1)
- CHF & Cardiac ArrestDocument12 pagesCHF & Cardiac ArrestRadhika BirlaNo ratings yet
- Heart Transplant ContentDocument17 pagesHeart Transplant ContentrajNo ratings yet
- Coronary Artery Bypass Graph Concept MapDocument5 pagesCoronary Artery Bypass Graph Concept Mapnursing concept maps100% (1)
- Bahan Askep Dekompensasi Kordis 2Document15 pagesBahan Askep Dekompensasi Kordis 2mulhayana yanaNo ratings yet
- HF Management GuideDocument49 pagesHF Management GuideJabraan Jamil100% (1)
- 10) Dyspnea Nov 2016 PDFDocument99 pages10) Dyspnea Nov 2016 PDFGopala HariNo ratings yet
- Manage Cor Pulmonale with Oxygen, Meds & Lifestyle ChangesDocument29 pagesManage Cor Pulmonale with Oxygen, Meds & Lifestyle ChangesdaisyNo ratings yet
- Guide to Canine and Feline ElectrocardiographyFrom EverandGuide to Canine and Feline ElectrocardiographyRuth WillisNo ratings yet
- Clinical Case - 1Document51 pagesClinical Case - 1Moush AbdiNo ratings yet
- Pharmacotherapy of heart failureDocument79 pagesPharmacotherapy of heart failureAbera JamboNo ratings yet
- 9, CHF BestDocument43 pages9, CHF BestauNo ratings yet
- Innovation in Clinical Care in Heart FailureDocument107 pagesInnovation in Clinical Care in Heart FailureSebastian Henao ErazoNo ratings yet
- Effects of Cardiac Problems On Individuals Functions of The Cardiac SystemDocument9 pagesEffects of Cardiac Problems On Individuals Functions of The Cardiac SystemJulie Nix FrazierNo ratings yet
- Kebutuhan Dasar Manusia OksigenasiDocument117 pagesKebutuhan Dasar Manusia Oksigenasiintanputri ramadhaniNo ratings yet
- Decompensatio Cordis: Disusun Oleh: Andi Rizky Fatir 2010730122 Pembimbing: Dr. Toton Suryotono Sp. PDDocument17 pagesDecompensatio Cordis: Disusun Oleh: Andi Rizky Fatir 2010730122 Pembimbing: Dr. Toton Suryotono Sp. PDHuda KamalNo ratings yet
- KP 2.5.5.1 Gagal Jantung KronikDocument39 pagesKP 2.5.5.1 Gagal Jantung Kronikayam kecapNo ratings yet
- Cardiac Failure & Myocardial Infarction GuideDocument6 pagesCardiac Failure & Myocardial Infarction GuideDaniel GeduquioNo ratings yet
- EHB 2015 Paper 157Document4 pagesEHB 2015 Paper 157Cringuta ParaschivNo ratings yet
- Anatomical and Physiological Overview of The HeartDocument45 pagesAnatomical and Physiological Overview of The Heartعمار المعمريNo ratings yet
- Valvular Heart Disease and Anesthesia Considerations for Non-Cardiac SurgeryDocument44 pagesValvular Heart Disease and Anesthesia Considerations for Non-Cardiac SurgeryLakshmi YalavarthyNo ratings yet
- Cardiac - Potpourri Rev 2015Document80 pagesCardiac - Potpourri Rev 2015Sanaz NikiNo ratings yet
- Neuromuscular and Other Diseases of The Chest WallDocument25 pagesNeuromuscular and Other Diseases of The Chest WallluckyNo ratings yet
- Heart Failure: Zelalem T., MD Yr III Resident, PediatricsDocument65 pagesHeart Failure: Zelalem T., MD Yr III Resident, PediatricsChalie MequanentNo ratings yet
- Patofisiologi Sistem KardiovaskularDocument157 pagesPatofisiologi Sistem KardiovaskularNyanmaruNo ratings yet
- Case study of Anterior Wall MIDocument32 pagesCase study of Anterior Wall MIسوما الشمريNo ratings yet
- Case 3Document9 pagesCase 3Maryam Shoukat AliNo ratings yet
- Left Ventricular FailureDocument17 pagesLeft Ventricular Failurenisha24100% (1)
- Atrial Fibrilation (AF) : Moh Gilang Fajriansyah Nohu (C11110285)Document38 pagesAtrial Fibrilation (AF) : Moh Gilang Fajriansyah Nohu (C11110285)GilankNo ratings yet
- Ischemic StrokeDocument20 pagesIschemic StrokeMargaret BaleNo ratings yet
- Cirrhotic CardiomyopathyDocument17 pagesCirrhotic CardiomyopathyVikasYellapuNo ratings yet
- Cardiogenic Shock GRP 2Document28 pagesCardiogenic Shock GRP 2LeeyanBhadzzVagayNo ratings yet
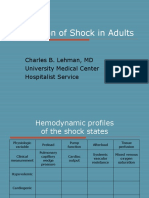
- Evaluation of Hemodynamic Profiles in Shock StatesDocument99 pagesEvaluation of Hemodynamic Profiles in Shock StatesekramsNo ratings yet
- Heart Failure in ChildrenDocument44 pagesHeart Failure in ChildrenRisna Ariani100% (2)
- CARDIOVASCULAR DISEASES: SIGNS, SYMPTOMS AND TREATMENT OF HEART FAILUREDocument27 pagesCARDIOVASCULAR DISEASES: SIGNS, SYMPTOMS AND TREATMENT OF HEART FAILURESanthoshi Sadhanaa SankarNo ratings yet
- CHFDocument35 pagesCHFMarione GimenezNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- 2017-Issues of Acute Kidney Injury Staging and Management in Sepsis and Critical Illness A Narrative Review PDFDocument25 pages2017-Issues of Acute Kidney Injury Staging and Management in Sepsis and Critical Illness A Narrative Review PDFClaudioLagosNo ratings yet
- Hypokalemi Dan AMIDocument4 pagesHypokalemi Dan AMIEnvhy AmaliaNo ratings yet
- Epidemiologi Penyakit Jantung & Pembuluh Darah: Oleh: Dr. Santi Martini, DR., M.Kes. Departemen Epidemiologi FKM UnairDocument42 pagesEpidemiologi Penyakit Jantung & Pembuluh Darah: Oleh: Dr. Santi Martini, DR., M.Kes. Departemen Epidemiologi FKM UnairAfif KunaifiNo ratings yet
- Katarak JurnalDocument9 pagesKatarak Jurnalmichelle1945No ratings yet
- BedahDocument57 pagesBedahBella OktavianiNo ratings yet
- Which One in TheDocument5 pagesWhich One in TheEnvhy AmaliaNo ratings yet
- CBE PrReDocument18 pagesCBE PrReEnvhy AmaliaNo ratings yet
- Acute Coronary Syndrome: Carrie Hurst FY1Document28 pagesAcute Coronary Syndrome: Carrie Hurst FY1Envhy AmaliaNo ratings yet
- Ucm 456073Document43 pagesUcm 456073Envhy AmaliaNo ratings yet
- Principles of Anatomy and Physiology: The Reproductive SystemsDocument52 pagesPrinciples of Anatomy and Physiology: The Reproductive SystemsEnvhy AmaliaNo ratings yet
- Dengue Fever Information SheetDocument2 pagesDengue Fever Information SheetEnvhy AmaliaNo ratings yet
- 17 22 Tingkat Pengetahuan Remaja Putri Kelas Xi Tentang Fibroadenoma Mammae Di Sma Masehi KudusDocument6 pages17 22 Tingkat Pengetahuan Remaja Putri Kelas Xi Tentang Fibroadenoma Mammae Di Sma Masehi KudusnatzevaraNo ratings yet
- Profiles and Outcomes of Head Injury at Nakuru Level 5 HospitalDocument5 pagesProfiles and Outcomes of Head Injury at Nakuru Level 5 HospitalEnvhy AmaliaNo ratings yet
- Unit 1 - Breast Anatomy and PhysiologyDocument50 pagesUnit 1 - Breast Anatomy and PhysiologyClyde R.OrtegaNo ratings yet
- Austin Neurosurgery: Open AccessDocument2 pagesAustin Neurosurgery: Open AccessAustin Publishing GroupNo ratings yet
- Cardiac Arrhythmia Resident 06Document56 pagesCardiac Arrhythmia Resident 06Envhy AmaliaNo ratings yet
- Unit 1 - Breast Anatomy and PhysiologyDocument50 pagesUnit 1 - Breast Anatomy and PhysiologyClyde R.OrtegaNo ratings yet
- Acute Coronary Syndrome: Carrie Hurst FY1Document28 pagesAcute Coronary Syndrome: Carrie Hurst FY1Envhy AmaliaNo ratings yet
- Brain Sciences: Pathophysiology and Imaging Diagnosis of Demyelinating DisordersDocument3 pagesBrain Sciences: Pathophysiology and Imaging Diagnosis of Demyelinating DisordersEnvhy AmaliaNo ratings yet
- Austin Neurosurgery: Open AccessDocument2 pagesAustin Neurosurgery: Open AccessAustin Publishing GroupNo ratings yet
- Cardiac Arrhythmia Resident 06Document56 pagesCardiac Arrhythmia Resident 06Envhy AmaliaNo ratings yet
- Kidneys and Kidney DiseaseDocument4 pagesKidneys and Kidney DiseaseArtscmNo ratings yet
- The Association Between Metaplasia and Gastric Malignancy With Helicobater Pylori InfectionDocument4 pagesThe Association Between Metaplasia and Gastric Malignancy With Helicobater Pylori InfectionEnvhy AmaliaNo ratings yet
- 2014 NSTE ACS Slide SetDocument109 pages2014 NSTE ACS Slide SetmikaNo ratings yet
- Coding Guidelines PDFDocument4 pagesCoding Guidelines PDFMystic TravellerNo ratings yet
- Afzal N, Anjum R, Nadeem A, Javed K, Shahzad F, Kashif M, Zafar A, Zaman S, Nagi AHDocument5 pagesAfzal N, Anjum R, Nadeem A, Javed K, Shahzad F, Kashif M, Zafar A, Zaman S, Nagi AHEnvhy AmaliaNo ratings yet
- Original Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsDocument6 pagesOriginal Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsEnvhy AmaliaNo ratings yet
- Study of Association of Thrombocytopenia With Plasmodium Vivax Infection Other Infections Original ArticleDocument3 pagesStudy of Association of Thrombocytopenia With Plasmodium Vivax Infection Other Infections Original ArticleEnvhy AmaliaNo ratings yet
- Human Cannibalism 1Document8 pagesHuman Cannibalism 1api-409100981No ratings yet
- Health Promotion and Disease Prevention in the ElderlyDocument1 pageHealth Promotion and Disease Prevention in the ElderlyBeverly PagcaliwaganNo ratings yet
- Emropub 2016 en 19266Document45 pagesEmropub 2016 en 19266jamshaidjiNo ratings yet
- Wound Care InstructionsDocument3 pagesWound Care InstructionsKat TaasinNo ratings yet
- Nur 097 Sas 1 3Document9 pagesNur 097 Sas 1 3gekkonoojiNo ratings yet
- Physiology of Sleep: Michael Schupp MD FRCA Christopher D Hanning MD FRCADocument6 pagesPhysiology of Sleep: Michael Schupp MD FRCA Christopher D Hanning MD FRCArichie_ciandraNo ratings yet
- MalariaDocument4 pagesMalarianafrabNo ratings yet
- Kim (2015) - Lemon Detox Diet Reduced Body FatDocument12 pagesKim (2015) - Lemon Detox Diet Reduced Body FatRodrigo MelloNo ratings yet
- Standards of Care in Child Care InstitutionsDocument36 pagesStandards of Care in Child Care InstitutionsVaishnavi JayakumarNo ratings yet
- Clinical Procedures For Medical Assistants 9th Edition Bonewit Test BankDocument12 pagesClinical Procedures For Medical Assistants 9th Edition Bonewit Test Bankcarriejordanwboriaqmfn100% (16)
- TB PDFDocument12 pagesTB PDFHana AshrafNo ratings yet
- Pteridophytes MorphologyDocument79 pagesPteridophytes MorphologyBoopathiAyyanarMNo ratings yet
- Test-11 (Current Affair-2)Document86 pagesTest-11 (Current Affair-2)Pavansaikumar DasariNo ratings yet
- Managing Hatch Rate and Diseases in Catfish EggsDocument6 pagesManaging Hatch Rate and Diseases in Catfish Eggsapi-3737467No ratings yet
- Cystic HygromaDocument12 pagesCystic Hygromaraymond onyekaNo ratings yet
- Daftar Pustaka HipertensiDocument43 pagesDaftar Pustaka HipertensiFeni Nurmia PutriNo ratings yet
- Anti-Rabies Act of 2007 (Ra 9482) 2Document29 pagesAnti-Rabies Act of 2007 (Ra 9482) 2Ronz Rogan100% (1)
- Radiology Report-R5016547Document4 pagesRadiology Report-R5016547Rajeev SNo ratings yet
- Disease Prediction Using Machine LearningDocument10 pagesDisease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Neuromuscular Therapy Techniques for Stroke and MS RehabilitationDocument11 pagesNeuromuscular Therapy Techniques for Stroke and MS RehabilitationWenzy Razzie cruzNo ratings yet
- Indian Herbs Cooking GuideDocument37 pagesIndian Herbs Cooking Guidehitesh mendirattaNo ratings yet
- Renal Vegetarian NutritionDocument2 pagesRenal Vegetarian NutritionSg Balaji100% (1)
- The Race Myth (Excerpted)Document30 pagesThe Race Myth (Excerpted)Wayne Owen Richards100% (1)
- Programs of Doh - NCDDocument71 pagesPrograms of Doh - NCDZOVELLA AURORA M. ACURAMNo ratings yet
- Routine Use of Vitamin K in The Treatment of Cirrhosis-Related Coagulopathy: Is It A-O-K? Maybe Not, We SayDocument6 pagesRoutine Use of Vitamin K in The Treatment of Cirrhosis-Related Coagulopathy: Is It A-O-K? Maybe Not, We Sayannisa edwarNo ratings yet
- Section 5 - Students WorksheetDocument4 pagesSection 5 - Students WorksheetEsraa AhmedNo ratings yet
- Session 14 Anxiety - Related DisordersDocument1 pageSession 14 Anxiety - Related DisordersMichelle Dona MirallesNo ratings yet
- 1.A Ndera CaseDocument13 pages1.A Ndera CaseNsengimana Eric MaxigyNo ratings yet
- Angina Pectoris: Dr. Naitik D Trivedi & Dr. Upama N. TrivediDocument15 pagesAngina Pectoris: Dr. Naitik D Trivedi & Dr. Upama N. TrivediNaveen KumarNo ratings yet
- USMLE Step 1 NBME Top Concepts 2021Document475 pagesUSMLE Step 1 NBME Top Concepts 2021dalia khamoNo ratings yet