You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Factors Affecting Job Satisfaction of EngineersDocument35 pagesFactors Affecting Job Satisfaction of Engineerslingg8850% (2)
- Canyon Colorado Electrical Body Builders Manual Service Manual 2015 en USDocument717 pagesCanyon Colorado Electrical Body Builders Manual Service Manual 2015 en USAlbertiniCongoraAsto100% (1)
- Six Petals of Peace DiscussionDocument10 pagesSix Petals of Peace Discussionjofel delicana100% (2)
- Team Roles EssayDocument7 pagesTeam Roles EssayCecilie Elisabeth KristensenNo ratings yet
- Bladder Carsinomas: Azif Zilal FauqiDocument18 pagesBladder Carsinomas: Azif Zilal FauqikadinfathiaNo ratings yet
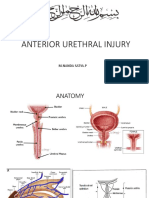
- Rupture Urethra Anterior DR Sule FixDocument36 pagesRupture Urethra Anterior DR Sule FixkadinfathiaNo ratings yet
- Stem Cell ArticleDocument6 pagesStem Cell ArticlekadinfathiaNo ratings yet
- Journal Reading: "Endothelial Function and Inflammation in Coronary Artery Disease"Document18 pagesJournal Reading: "Endothelial Function and Inflammation in Coronary Artery Disease"kadinfathiaNo ratings yet
- Jurnal KulitDocument24 pagesJurnal KulitkadinfathiaNo ratings yet
- EnglishDocument9 pagesEnglishkadinfathiaNo ratings yet
- OphthalmologyDocument22 pagesOphthalmologykadinfathia0% (1)
- Materi RTD Bagian: Co-Ass AnestesiDocument3 pagesMateri RTD Bagian: Co-Ass AnestesikadinfathiaNo ratings yet
- Journal Reading: "Endothelial Function and Inflammation in Coronary Artery Disease"Document18 pagesJournal Reading: "Endothelial Function and Inflammation in Coronary Artery Disease"kadinfathiaNo ratings yet
- Relationship between midwife characteristics and MCH service behaviorDocument1 pageRelationship between midwife characteristics and MCH service behaviorkadinfathiaNo ratings yet
- Lower Respiratory SystemDocument27 pagesLower Respiratory SystemkadinfathiaNo ratings yet
- Tests of NormalityDocument18 pagesTests of NormalitykadinfathiaNo ratings yet
- Translate Jurnal KeratitisDocument7 pagesTranslate Jurnal KeratitiskadinfathiaNo ratings yet
- Exogenous Ochronosis With Use of Low Potency Hydroquinone in A Caucasian PatientDocument27 pagesExogenous Ochronosis With Use of Low Potency Hydroquinone in A Caucasian PatientkadinfathiaNo ratings yet
- Sensus Pasien Anak Rsud K.R.M.T Wongsonegoro: Belum Visite Sudah Visite Belum Visite Sudah VisiteDocument2 pagesSensus Pasien Anak Rsud K.R.M.T Wongsonegoro: Belum Visite Sudah Visite Belum Visite Sudah VisitekadinfathiaNo ratings yet
- Luas Area EndometriosisDocument4 pagesLuas Area EndometriosiskadinfathiaNo ratings yet
- Antibiotics: January 2015Document35 pagesAntibiotics: January 2015kadinfathiaNo ratings yet
- ASTRO IPSS and SHIM Score Trends in Prostate Cancer Patients After IMRT PDFDocument1 pageASTRO IPSS and SHIM Score Trends in Prostate Cancer Patients After IMRT PDFkadinfathiaNo ratings yet
- Farmakologi Obat AntibiotikDocument27 pagesFarmakologi Obat AntibiotikRecofol100% (1)
- Dsa510 PDFDocument22 pagesDsa510 PDFkadinfathiaNo ratings yet
- Iron THTDocument4 pagesIron THTkadinfathiaNo ratings yet
- ASTRO IPSS and SHIM Score Trends in Prostate Cancer Patients After IMRT PDFDocument1 pageASTRO IPSS and SHIM Score Trends in Prostate Cancer Patients After IMRT PDFkadinfathiaNo ratings yet
- I-PSS Prostate Symptom ScoreDocument2 pagesI-PSS Prostate Symptom ScoreFrida AnggaNo ratings yet
- Antibiotics: January 2015Document35 pagesAntibiotics: January 2015kadinfathiaNo ratings yet
- Jurnal TranslateDocument13 pagesJurnal TranslatekadinfathiaNo ratings yet
- List Perpus RadiologiDocument2 pagesList Perpus RadiologikadinfathiaNo ratings yet
- Definisi, Epidemiologi, Klasifikasi, dan Terapi Karsinoma HepatokelularDocument37 pagesDefinisi, Epidemiologi, Klasifikasi, dan Terapi Karsinoma HepatokelularkadinfathiaNo ratings yet
- Speech About SDGs HealthDocument2 pagesSpeech About SDGs HealthkadinfathiaNo ratings yet
- Definisi, Epidemiologi, Klasifikasi, dan Terapi Karsinoma HepatokelularDocument37 pagesDefinisi, Epidemiologi, Klasifikasi, dan Terapi Karsinoma HepatokelularkadinfathiaNo ratings yet
- San Mateo Daily Journal 05-06-19 EditionDocument28 pagesSan Mateo Daily Journal 05-06-19 EditionSan Mateo Daily JournalNo ratings yet
- UNIT 1 Sociology - Lisening 2 Book Review of Blink by Malcolm GladwellDocument9 pagesUNIT 1 Sociology - Lisening 2 Book Review of Blink by Malcolm GladwellNgọc ÁnhNo ratings yet
- Application Performance Management Advanced For Saas Flyer PDFDocument7 pagesApplication Performance Management Advanced For Saas Flyer PDFIrshad KhanNo ratings yet
- REMEDIOS NUGUID vs. FELIX NUGUIDDocument1 pageREMEDIOS NUGUID vs. FELIX NUGUIDDanyNo ratings yet
- American Wire & Cable Daily Rated Employees Union v. American Wire & Cable Co and Court of AppealsDocument2 pagesAmerican Wire & Cable Daily Rated Employees Union v. American Wire & Cable Co and Court of AppealsFoxtrot Alpha100% (1)
- Prep - VN: Where Did The Polo Family Come From?Document1 pagePrep - VN: Where Did The Polo Family Come From?Phương LanNo ratings yet
- Human Resource Development's Evaluation in Public ManagementDocument9 pagesHuman Resource Development's Evaluation in Public ManagementKelas KP LAN 2018No ratings yet
- 12A1HDocument11 pages12A1HAlvaro SolisNo ratings yet
- NetZoom Pro v15 Install GuideDocument81 pagesNetZoom Pro v15 Install Guidescribd!!No ratings yet
- Elliptic FunctionsDocument66 pagesElliptic FunctionsNshuti Rene FabriceNo ratings yet
- UAE Cooling Tower Blow DownDocument3 pagesUAE Cooling Tower Blow DownRamkiNo ratings yet
- FOL Predicate LogicDocument23 pagesFOL Predicate LogicDaniel Bido RasaNo ratings yet
- Criteria For RESEARCHDocument8 pagesCriteria For RESEARCHRalph Anthony ApostolNo ratings yet
- Future42 1675898461Document48 pagesFuture42 1675898461Rodrigo Garcia G.No ratings yet
- Senior Civil Structure Designer S3DDocument7 pagesSenior Civil Structure Designer S3DMohammed ObaidullahNo ratings yet
- Airforce Group Y: Previous Y Ear P AperDocument14 pagesAirforce Group Y: Previous Y Ear P Aperajay16duni8No ratings yet
- Balochistan Conservation Strategy VDocument388 pagesBalochistan Conservation Strategy VHãšãñ Trq100% (1)
- Syllabus For The Post of ASI - Traffic - WardensDocument2 pagesSyllabus For The Post of ASI - Traffic - WardensUbaid KhanNo ratings yet
- Cell Types: Plant and Animal TissuesDocument40 pagesCell Types: Plant and Animal TissuesMARY ANN PANGANNo ratings yet
- Reduce Home Energy Use and Recycling TipsDocument4 pagesReduce Home Energy Use and Recycling Tipsmin95No ratings yet
- Gcu On Wiki PediaDocument10 pagesGcu On Wiki Pediawajid474No ratings yet
- Solar Presentation – University of Texas Chem. EngineeringDocument67 pagesSolar Presentation – University of Texas Chem. EngineeringMardi RahardjoNo ratings yet
- Mr. Bill: Phone: 086 - 050 - 0379Document23 pagesMr. Bill: Phone: 086 - 050 - 0379teachererika_sjcNo ratings yet
- Lucy Wang Signature Cocktail List: 1. Passion Martini (Old Card)Document5 pagesLucy Wang Signature Cocktail List: 1. Passion Martini (Old Card)Daca KloseNo ratings yet
- Zeng 2020Document11 pagesZeng 2020Inácio RibeiroNo ratings yet
- Preterm Labour: Muhammad Hanif Final Year MBBSDocument32 pagesPreterm Labour: Muhammad Hanif Final Year MBBSArslan HassanNo ratings yet