You might also like
- Fracture Condyle PDFDocument57 pagesFracture Condyle PDFDrShary Ann MathewNo ratings yet
- Nasal Fracture Reduction TechniquesDocument26 pagesNasal Fracture Reduction TechniquesSiti Hidayatul FitriNo ratings yet
- Dr. Faruly Wijaya S. Limba, SPB Rsu BahteramasDocument18 pagesDr. Faruly Wijaya S. Limba, SPB Rsu BahteramasZurezki Andezt YafiieeNo ratings yet
- Essay Blow Out Fracture - Rina Widia AstutiDocument8 pagesEssay Blow Out Fracture - Rina Widia AstutiRina Widia AstutiNo ratings yet
- Maxillofacial Trauma: PG TutorialDocument113 pagesMaxillofacial Trauma: PG TutorialChacha TasyaNo ratings yet
- Blowoutfractures PresentationDocument38 pagesBlowoutfractures PresentationVISHAKHANo ratings yet
- FX Max Orb Slides 2004 0107Document55 pagesFX Max Orb Slides 2004 0107tekoman01No ratings yet
- Maxillofacial TraumaDocument70 pagesMaxillofacial Traumaeman_879_123456No ratings yet
- Surgical Outcome of Blowout Fractures of Floor of Orbit A Case Series Of5 Patients 2155 9570 1000518Document5 pagesSurgical Outcome of Blowout Fractures of Floor of Orbit A Case Series Of5 Patients 2155 9570 1000518Luqman HakimNo ratings yet
- Nasal Fractures: Stephen Kinyanjui BDSC/ 4837/161/DFDocument56 pagesNasal Fractures: Stephen Kinyanjui BDSC/ 4837/161/DFStephen KinyanjuiNo ratings yet
- Mandibular FracturesDocument46 pagesMandibular FracturesAntony Sebastian100% (1)
- Nasal and Facial Fractures: DR - Imran Qazi Ent A Tmo KTH PeshawarDocument42 pagesNasal and Facial Fractures: DR - Imran Qazi Ent A Tmo KTH Peshawarimran qaziNo ratings yet
- Ophthalmological Injuries Associated With Fractures of The Orbitozygomaticomaxillary ComplexDocument32 pagesOphthalmological Injuries Associated With Fractures of The Orbitozygomaticomaxillary ComplexDR NASIMNo ratings yet
- Orbital Decompression, Optic N Decompression and EndoDCRDocument97 pagesOrbital Decompression, Optic N Decompression and EndoDCRAlok RathiNo ratings yet
- OtosclerosisDocument44 pagesOtosclerosisSonal Sharma100% (1)
- Ocular Trauma For Med VDocument58 pagesOcular Trauma For Med Vhenok birukNo ratings yet
- Management of Maxillofacial Trauma: Zygomatic Complex FracturesDocument50 pagesManagement of Maxillofacial Trauma: Zygomatic Complex FracturesShabeel PnNo ratings yet
- Tumor Flash Cards - Osteochondroma and Multiple Hereditary ExostosisDocument23 pagesTumor Flash Cards - Osteochondroma and Multiple Hereditary Exostosislaxge54No ratings yet
- Os Finals ReviewerDocument33 pagesOs Finals ReviewerGuen ColisNo ratings yet
- Mandibular FractresDocument37 pagesMandibular Fractresdileep900No ratings yet
- Mandibular FractresDocument37 pagesMandibular FractresSenthil NathanNo ratings yet
- Management of Mandibular FracturesDocument53 pagesManagement of Mandibular FracturesDenise Johnson75% (8)
- Zygomatic Complex Fractures: Classification, Management and ComplicationsDocument49 pagesZygomatic Complex Fractures: Classification, Management and ComplicationskikoNo ratings yet
- Management of Maxillofacial Trauma: Zygomatic Complex FracturesDocument50 pagesManagement of Maxillofacial Trauma: Zygomatic Complex Fracturesnoovy608829No ratings yet
- JEgyptOphthalmolSoc108247-3254949 090229Document5 pagesJEgyptOphthalmolSoc108247-3254949 090229ali alenziNo ratings yet
- CystotomyDocument34 pagesCystotomycrazieelorraNo ratings yet
- Musculosceletal Block: Prof - Dr.Dr. Bambang Pardjianto, SPB., Spbp-Re (K)Document32 pagesMusculosceletal Block: Prof - Dr.Dr. Bambang Pardjianto, SPB., Spbp-Re (K)Irsyad Robani WNo ratings yet
- Ocular TraumaDocument67 pagesOcular TraumaRenita Siwi M WNo ratings yet
- Orbitalfractures: Kris S. Moe,, Andrew H. Murr,, Sara Tullis WesterDocument15 pagesOrbitalfractures: Kris S. Moe,, Andrew H. Murr,, Sara Tullis Westerstoia_sebiNo ratings yet
- ABGD Study Guide 2009Document443 pagesABGD Study Guide 2009velangniNo ratings yet
- Final ExamDocument30 pagesFinal ExamYoussef ElbeharyNo ratings yet
- Capps 9.18.07 W ExtraDocument69 pagesCapps 9.18.07 W Extrasamuel.fang3434No ratings yet
- Apert Syndrome - Sultan BaroamaimDocument37 pagesApert Syndrome - Sultan BaroamaimsultanNo ratings yet
- General Principles of FractureDocument31 pagesGeneral Principles of Fractureamel015No ratings yet
- Facial Plastic Surgery Clinics of North America Volume 14, Issue 1, Pages 1-62 (February 2006), Endoscopic Craniomaxillofacial SurgeryDocument62 pagesFacial Plastic Surgery Clinics of North America Volume 14, Issue 1, Pages 1-62 (February 2006), Endoscopic Craniomaxillofacial SurgeryConstellatus Cornelius100% (3)
- Lect 8 - Internal Fixation - IIDocument21 pagesLect 8 - Internal Fixation - IIAnkit LakshyaNo ratings yet
- The Periodontal FlapDocument37 pagesThe Periodontal FlapPrathik RaiNo ratings yet
- Fractures of The Zygomatic Complex LecDocument16 pagesFractures of The Zygomatic Complex LecFarhan KhanNo ratings yet
- Mandible FracturesDocument60 pagesMandible FracturesMellow MenaisNo ratings yet
- Zygomatic Arch and Orbital FracturesDocument6 pagesZygomatic Arch and Orbital FractureszacrouchyNo ratings yet
- Panfacial TraumaDocument104 pagesPanfacial TraumaMehek BatraNo ratings yet
- Maxillary Sinus Lifting: 10.5005/jp-Journals-10029-1181Document7 pagesMaxillary Sinus Lifting: 10.5005/jp-Journals-10029-1181Mohammad HarrisNo ratings yet
- Periodontal Surgery Biological WidthDocument7 pagesPeriodontal Surgery Biological WidthhunarsandhuNo ratings yet
- Management of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportDocument6 pagesManagement of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportIma ShofyaNo ratings yet
- Facial Trauma: Joni Skipper, MS-IV USC School of MedicineDocument22 pagesFacial Trauma: Joni Skipper, MS-IV USC School of Medicinealma23roNo ratings yet
- Facial Trauma Diagnosis and TreatmentDocument22 pagesFacial Trauma Diagnosis and TreatmentReggy Amalia NurgammaNo ratings yet
- Femur Fxby TahirDocument77 pagesFemur Fxby Tahirtahir mahmood100% (1)
- Tear Dropsign Vs FractureDocument10 pagesTear Dropsign Vs FractureDeepak AnNo ratings yet
- Section 018 Pre Prosthetic Surgery 1Document21 pagesSection 018 Pre Prosthetic Surgery 1Sherry AndrewsNo ratings yet
- Advancesinthe Reconstructionoforbital Fractures: Scott E. Bevans,, Kris S. MoeDocument23 pagesAdvancesinthe Reconstructionoforbital Fractures: Scott E. Bevans,, Kris S. Moestoia_sebiNo ratings yet
- ZMC Fracture in Oral SurgeryDocument60 pagesZMC Fracture in Oral SurgeryRiya Correa0% (1)
- Open Fractures of The Tibial Diaphysis: David Templeman, MD Darin Friess, MDDocument50 pagesOpen Fractures of The Tibial Diaphysis: David Templeman, MD Darin Friess, MDDwi Tantri SPNo ratings yet
- 11.Endodontic MishapsDocument27 pages11.Endodontic MishapsRiya JainNo ratings yet
- Presentasi Fraktur FKK UMJDocument102 pagesPresentasi Fraktur FKK UMJIndahNovikaNo ratings yet
- Blow Out Fracture: Ocular EmergencyDocument5 pagesBlow Out Fracture: Ocular EmergencyMeyrani 'andiz' SilviaNo ratings yet
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionFrom EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionRating: 4 out of 5 stars4/5 (1)
- The MeniscusFrom EverandThe MeniscusPhilippe BeaufilsNo ratings yet
- Purpose of LifeDocument40 pagesPurpose of LifeShabeel PnNo ratings yet
- Border-Molding in Complete DentureDocument40 pagesBorder-Molding in Complete DentureShabeel Pn100% (14)
- Apexion Dental Products and ServicesDocument1 pageApexion Dental Products and ServicesShabeel PnNo ratings yet
- Otitis MediaDocument42 pagesOtitis MediaShabeel PnNo ratings yet
- Gram-Negative SEPSISDocument59 pagesGram-Negative SEPSISShabeel PnNo ratings yet
- Management of Maxillofacial Trauma: Zygomatic Complex FracturesDocument50 pagesManagement of Maxillofacial Trauma: Zygomatic Complex FracturesShabeel PnNo ratings yet
- Trauma - in DetailDocument67 pagesTrauma - in DetailShabeel PnNo ratings yet
- Acute SinusitisDocument42 pagesAcute SinusitisShabeel PnNo ratings yet
- TracheostomyDocument40 pagesTracheostomyShabeel PnNo ratings yet
- Surgical InfectionsDocument45 pagesSurgical InfectionsShabeel PnNo ratings yet
- Guidelines For Emergency TracheostomyDocument41 pagesGuidelines For Emergency TracheostomyShabeel PnNo ratings yet
- HyperparathyroidismDocument41 pagesHyperparathyroidismShabeel PnNo ratings yet
- Implant Supported Fixed ProsthesisDocument32 pagesImplant Supported Fixed ProsthesisShabeel PnNo ratings yet
- CSF LeaksDocument34 pagesCSF LeaksShabeel PnNo ratings yet
- Maxillofacial, Ophthalmic & Dental TraumaDocument31 pagesMaxillofacial, Ophthalmic & Dental TraumaShabeel PnNo ratings yet
- Dental Tourism: Presented by DR Shabeel PNDocument17 pagesDental Tourism: Presented by DR Shabeel PNShabeel PnNo ratings yet
- Dento Alveolar FracturesDocument16 pagesDento Alveolar FracturesShabeel PnNo ratings yet
- OsseointegrationDocument36 pagesOsseointegrationShabeel Pn100% (1)
- Dental InstrumentsDocument14 pagesDental InstrumentsShabeel PnNo ratings yet
- Oral Health and NutritionDocument36 pagesOral Health and NutritionShabeel PnNo ratings yet
- Glass Ionomer CementDocument135 pagesGlass Ionomer CementShabeel PnNo ratings yet
- Oral and Maxillofacial SurgeonsDocument15 pagesOral and Maxillofacial SurgeonsShabeel PnNo ratings yet
- Working Casts and Die SystemsDocument45 pagesWorking Casts and Die SystemsShabeel Pn100% (1)
- Dental Anatomy: DR Shabeel 1Document40 pagesDental Anatomy: DR Shabeel 1Shabeel PnNo ratings yet
- Diabetes Mellitus PatientsDocument33 pagesDiabetes Mellitus PatientsShabeel PnNo ratings yet
- Prevetion of Dental CariesDocument76 pagesPrevetion of Dental CariesShabeel PnNo ratings yet
- Detecting Oral Cancer: Dentfinishingschool - BlogspDocument29 pagesDetecting Oral Cancer: Dentfinishingschool - BlogspShabeel PnNo ratings yet
- BLOOD CoagulationDocument43 pagesBLOOD CoagulationShabeel PnNo ratings yet
- Child PsychologyDocument25 pagesChild PsychologyShabeel PnNo ratings yet
- Current Examination Methods of The Canine Eye: J. Beránek, P.J. VítDocument6 pagesCurrent Examination Methods of The Canine Eye: J. Beránek, P.J. VítOktavia firnandaNo ratings yet
- Management of Traumatic Iridodialysis with HyphaemaDocument21 pagesManagement of Traumatic Iridodialysis with HyphaemaSyed NabilNo ratings yet
- Global and Regional PrevalenceDocument13 pagesGlobal and Regional PrevalenceMacarena AlvarezNo ratings yet
- Form 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical FitnessDocument1 pageForm 1-A (See Rules 5 (1), (3), 7,10 (A), 14 (D), and 18 (D) ) : Certificate of Medical Fitnessamit kargwalNo ratings yet
- Thyroid Eye DiseaseDocument32 pagesThyroid Eye DiseaseGiorgos MousterisNo ratings yet
- OphthBusinessApril 2010 PDFDocument27 pagesOphthBusinessApril 2010 PDFDana Andreea PopescuNo ratings yet
- Risk Assessment For Installation and Testing of CCTVDocument11 pagesRisk Assessment For Installation and Testing of CCTVAnandu Ashokan100% (3)
- Effects of Progressive Addition Lens Wear On Digital Work in Pre-Presbyopes 4Document11 pagesEffects of Progressive Addition Lens Wear On Digital Work in Pre-Presbyopes 4Valentina PereaNo ratings yet
- Dutta 3Document601 pagesDutta 3Jeel GaralaNo ratings yet
- SL 220 User ManualDocument68 pagesSL 220 User Manualdummy account100% (1)
- The International Workshop On Meibomian GlandDocument44 pagesThe International Workshop On Meibomian GlandPutri kartiniNo ratings yet
- Family Case Week 3Document25 pagesFamily Case Week 3Luiezt BernardoNo ratings yet
- Operasi Dakriosistorhinostomi DCR Pada Pasien Dengan Dakriosistitis Kronis - Novaqua YandiDocument13 pagesOperasi Dakriosistorhinostomi DCR Pada Pasien Dengan Dakriosistitis Kronis - Novaqua YandiIDI Bangka BaratNo ratings yet
- Drugs For Eye and Ear DisordersDocument4 pagesDrugs For Eye and Ear DisordersApple MaeNo ratings yet
- As ISO 11979.6-2003 Opthalmic Implants - Intraocular Lenses Shelf-Life and Transport StabilityDocument8 pagesAs ISO 11979.6-2003 Opthalmic Implants - Intraocular Lenses Shelf-Life and Transport StabilitySAI Global - APACNo ratings yet
- Aravind Eye Care System-Case StudyDocument21 pagesAravind Eye Care System-Case StudyAbhinav MalikNo ratings yet
- TG 6 Refractive ErrorDocument11 pagesTG 6 Refractive ErrorNovi AdriNo ratings yet
- Task Risk Assessment Engineering Kinetics (PVT.) LTD: Risk Evaluation (Refer To Evaluation Form)Document3 pagesTask Risk Assessment Engineering Kinetics (PVT.) LTD: Risk Evaluation (Refer To Evaluation Form)andreNo ratings yet
- Emergency Contact Information: Your Name Address City, State, Zip Telephone Special DirectionsDocument2 pagesEmergency Contact Information: Your Name Address City, State, Zip Telephone Special DirectionsVictor Hugo Calvanapón SalasNo ratings yet
- Expt3 Group3 Surname, First NameDocument3 pagesExpt3 Group3 Surname, First NameBlazy InhumangNo ratings yet
- 6 Middle Facial FracturesDocument29 pages6 Middle Facial FracturesYoussef ElbeharyNo ratings yet
- Exp 5..effect of Mydriatic and Miotic Drug On Rabbit Eye - LabmonkDocument6 pagesExp 5..effect of Mydriatic and Miotic Drug On Rabbit Eye - LabmonkSubodh ShahNo ratings yet
- Shantilal Shanghvi Foundation recruiting para medical staff for new eye hospitalDocument1 pageShantilal Shanghvi Foundation recruiting para medical staff for new eye hospitalSunil ShrivastavNo ratings yet
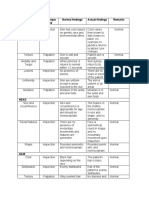
- Area Assessed Technique Used Normal Findings Actual Findings Remarks SkinDocument6 pagesArea Assessed Technique Used Normal Findings Actual Findings Remarks SkinLadybelle GototosNo ratings yet
- MANAJEMEN SERI KASUS RETINOPATI PREMATURITAS (ROPDocument15 pagesMANAJEMEN SERI KASUS RETINOPATI PREMATURITAS (ROPEko NoviantiNo ratings yet
- List of Emergency ContactsDocument6 pagesList of Emergency Contactsapi-26090714No ratings yet
- Calcium Carbonate MSDSDocument12 pagesCalcium Carbonate MSDSNinaNo ratings yet
- Article 4 Orthokeratology: An Update: Key WordsDocument8 pagesArticle 4 Orthokeratology: An Update: Key WordsLina Marcela FierroNo ratings yet
- Poly-F®: Zinc Polycarboxylate CementDocument11 pagesPoly-F®: Zinc Polycarboxylate CementNonoNo ratings yet
- Anaphy Lec Special SensesDocument6 pagesAnaphy Lec Special SensesRyan Dave UmayamNo ratings yet